Course Authors
Enoch B. Kassa, M.D., and Yang Sun, M.D., Ph.D.
Release Date: 01/11/2016
Upon completion of this Cyberounds®, you should be able to:
Discuss the epidemiology of cataract in both developed and developing countries;
Enumerate the risk factors of cataract formation;
Apply the epidemiology and risk factors to the management of patients with cataract.
Cataract is the leading cause of blindness in the world and it is responsible for an estimated 51% of world blindness, which represents about 20 million people.(1) Most patients in the western world undergo surgical replacement of the lens with a synthetic intra-ocular lens before significant vision loss occurs. Cataract surgery is the most commonly performed surgery in the United States.(2). Unfortunately, developing countries do not possess enough resources to provide vision-sparing surgeries for those with cataracts. Visual disability associated with cataract is significant in both developing and developed countries.(1) There is a higher prevalence of blindness caused by cataracts in developing countries.
The cataract is formed by the degeneration of the lens of the eye.(3) The main refractive structure within the eye, the lens allows transmission of light and focuses the light onto the retina. The lens fibers are long, thin and transparent bundles of tightly packed proteins that are surrounded by a capsule. During development, the lens forms from nucleated epithelial cells, which then extrude the nucleus and allow the proteins to pack within the capsular bag.
Age-related cataract formation causes gradual vision decline. While the exact mechanism of formation of cataracts is unknown, it is generally accepted that cataracts form because of protein denaturation and aggregation as a consequence of aging and environmental stresses.(3) UV light, smoking, diabetes, and surgical interventions are some of the known risk factors that accelerate cataract formation.(3) It is thought that these proteins aggregate because the lens does not have a way to get rid of damaged proteins.(4) Aggregation of proteins renders the proteins insoluble and decreases light transmission, leading to a visually significant cataract.
Despite major surgical advances to correct cataracts, non-surgical options remain nonexistent. Non-surgical treatments, if available, would benefit underserved regions that do not have the capabilities to perform surgeries.
Epidemiology
As the leading cause of blindness, cataracts develop with advancing age.(3) It is uncommon to develop cataract before age 40. Both genders are equally affected. Regions with high UV light exposure are affected at higher rates and at earlier ages(5) The 10-year incidence of cataracts is 54% in the US in people age 43 to 86 years. The highest incidence reported in the study was in Australia with 72% in people over the age 49.(2)
It is estimated that 20 million people are blind from cataracts in the world. The proportion is considerably higher in developing countries where specialized surgical management is not available. An epidemiologic study in a small village in Nigeria reported the burden of cataracts.(6) The 2005 projected population of Egbedore Local Government Area of Osun State, Nigeria, was 59,823 people, of whom 5,570 were adults aged 50 and older. The results of a population-based survey conducted in Egbedore indicated that 1.18% of the examined population of all age groups were bilaterally blind with visual acuity of less than 20/400. Of all blindness, 47.4% was caused by cataract.(6) Therefore, cataract presents a significant public health issue for both the developed and developing worlds.
Pathophysiology
Age-related cataract formation is caused by the denaturation of lens proteins.(3) The lens is made up of epithelial cells rich in cytoplasmic proteins. With age some of these lens cells degenerate and the denatured proteins initially cause distortion of light, which ultimately may result in complete blockage of light.
During aging, the lens becomes thickened and decreases its ability to refract light rays, likely the result of the increasing amounts of insoluble protein particles.(3) These proteins then form fibrils and accumulate as aggregated insoluble proteins leading to changes to the crystallin proteins of the lens causing clouding and refractive changes. In addition to covalent damages on crystallin proteins, genetic mutations in crystallin can also contribute to cataract formation. These abnormal crystallin proteins affect the solubility of the proteins leading to formation of aggregates.
The major risk factor for cataract formation is age. It is uncommon for young people to develop visually significant cataracts; rare syndromes and in-utero infections may result in congenital cataracts (not discussed here). Other risk factors include sunlight exposure, smoking, alcohol consumption and metabolic syndromes including diabetes. It is thought that any environmental stressor causing continuous damage to the lens contributes to cataract formation. Current smokers of more than 15 cigarettes per day had a 42% increased risk of cataract extraction (rate ratio, 1.42; 95% CI, 1.28-1.58) compared with never smokers after adjustment for age and other potential risk factors.(5) Smoking cessation significantly decreased the risk for cataract extraction with time (P < 0.001).
In the meta-analysis of 10 studies, the associations between moderate alcohol consumption and age-related cataract indicated that heavy alcohol consumption was associated with an increased risk of age-related cataract (pooled relative risk, 1.26; 95% confidence interval, 1.06 to 1.50; I = 58.9%).(8) Heavy alcohol consumption was defined as more than two standard drinks per day, which is equal to a daily intake of 20 g of alcohol or 140 g per week.
A retrospective study of 2852 subjects concluded that metabolic syndrome and its components, such as abdominal obesity, high blood pressure, and impaired fasting glucose, are associated with age-related cataract formation in the Korean population.(9) Men with metabolic syndrome had a 64% increased risk of nuclear cataract and women with metabolic syndrome had a 56% increased risk of cortical cataract. There was an overall 46-49% increased risk of developing any type of cataract in people with metabolic syndrome.
Secondary cataracts or acquired cataracts, as opposed to age-related cataracts, are caused by direct lens insult through infection, autoimmune illness and/or radiation therapy that causes crystallin protein destabilization. Therefore, ocular trauma, uveitis, scleritis, radiation exposure contribute to cataract formation.
Medications have been associated with cataract formation. The most common medication is corticosteroid. Patients on either topical or systemic corticosteroids are at higher risks for development of secondary cataracts. With the increasing use of corticosteroid in patients with inflammatory diseases, such as rheumatoid arthritis, there is corresponding rise in the medication-induced cataracts.
Presentation
Diagnosis of low vision due to cataract is made with both history and slit lamp examination. People with cataracts often present with a progressive decline in vision. Patients complain of a problem with low light vision especially during night driving, with oncoming headlights. Symptoms of glare, halos, and "sunbursts" are common initial complains. Patients will also report difficulty reading fine print because in many cases, the shape of the lens is altered, which exacerbates nearsightedness. This increase in refractive power is called myopic shift, which is generally corrected with spectacles. An age-related increase in glasses prescription strength can indicate progression of a cataract.
As the cataract progresses, the patients may complain of decreased color vision, noting bright objects appear dull in color. Decreased vision with daily activities such as reading of newspaper and watching television would affect the quality of life. Eventually, as the cataract becomes mature or opaque (brunescent cataract), the patient can become very disabled and may require assistance with self-care.
Using a specialized machine called a slit lamp, an eye physician can diagnose cataract by the degree of light obstruction in the lens. As the lens age, chemical modifications cause a progressive pigmentation and a yellowing of the nuclear lens. An excessive amount of yellowing and sclerosis results in a cataract formation, which is accompanied by decreased red reflex by direct ophthalmoscopy and reduced contrast of the retina by slit lamp examination.
Nuclear cataracts progressively deteriorate distance vision and contrast and lamellar cataracts are not as visually significant (Figure 1).

Figure 1.
Nuclear Sclerotic Cataract.
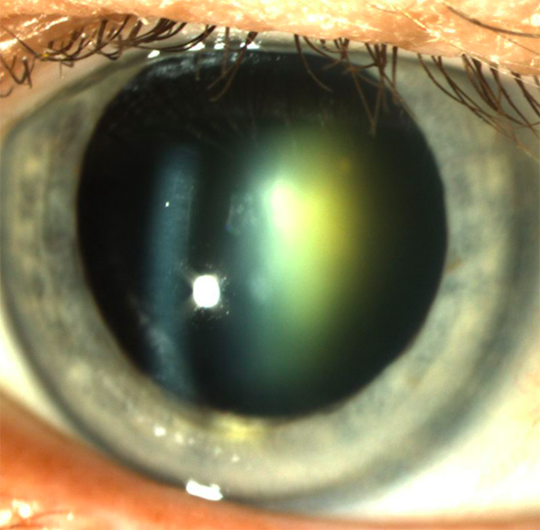
An age-related nuclear sclerotic cataract with yellowing hue of the lens.
Cortical cataract, another form commonly associated with age, typically do not cause decline in vision as much as nuclear opacities, but may cause double vision due to irregular light refraction (Figure 2).
Figure 2.
Cortical Cataract.
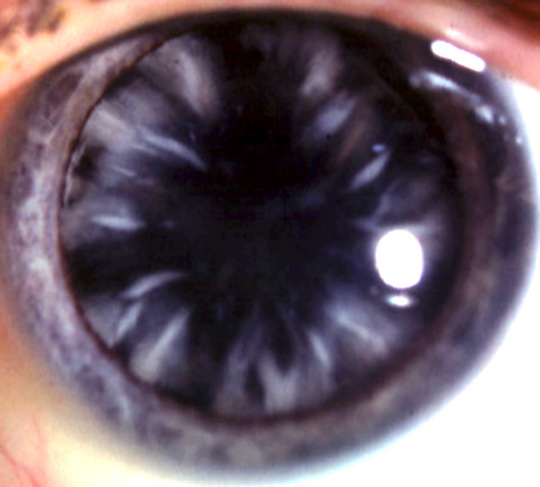
Cortical cataracts are a relatively common form of cataract which have radial wedge shapes at mid-depth in the cortex.
Another common form is the posterior capsular cataract, in which the posterior capsule of the lens can develop an opacity and can cause disabling glare (Figure 3); this form of cataract is more pronounced in both diabetic patients and steroid-induced cataracts.
Figure 3.
Subcapsular Cataract.
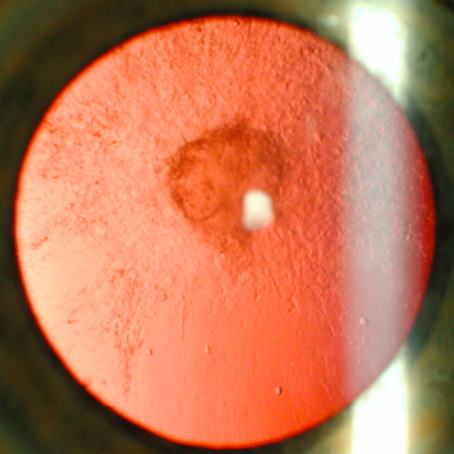
Posterior subcapsular cataract due to topical steroid use, as viewed with retroillumination.
During slit lamp examination, a nascent cataract allows a view of the retina and the physician will detect a red reflex during a fundoscopic exam. As the cataract progresses, a decreased red reflex is indicative of the progression and may indicate a need for cataract surgery. A mature cataract may result in legal blindness and the vision is usually worse than 20/400 (Figure 4). The most common indication for surgery, however, is a "visually significant" cataract, which may be subjective for each patient.
Figure 4.
Mature Cataract.
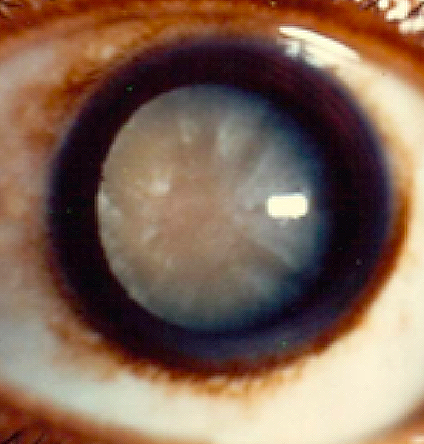
A mature cataract with opacified fibers and brunescent appearance.
Cataracts have significant socioeconomic and psychological effects. A recent quality of life questionnaire in 401 patients was performed to evaluate the effects of cataracts.(10) The study found that cataracts significantly decreased vision-related quality of life in most of the measured parameters. Mental health, role difficulty, general vision, near vision activities, and dependence were the most affected parameters. Because the mental health and role difficulty were classified as psychosocial parameters, the results also indicated that visual impairment had more impact on the psychosocial parameter than the other quality of life parameters. Greater visual impairment was significantly associated with lower subscale scores, which in turn predicted increased limitations in daily activities. These limitations can leads to a decrease in social interactions and an increase in dependence, further resulting in greater psychosocial symptoms.
Management
Currently there are no medical therapies to reverse the effects of a cataract. Reducing risk factors such as smoking, sun exposure, and corticosteroid exposure may help to delay the progression of cataracts.
At the beginning of cataracts, vision can be improved with a change in spectacles. As the cataract progresses, over the course of months to years, increasing the strength of prescription glasses will lose its effectiveness and cataract surgery will be required to restore vision. Similar to prescription glasses, intra-ocular lenses have specific power unique to the patient's eyes. There are several types of lenses available commercially and patients should choose which lens they prefer.
During cataract surgery, the inner lens material is removed and a new synthetic lens is placed. The surgical procedure is done as an outpatient service and patients can go home afterwards. While both eyes may need cataract surgeries, the first operation is on the eye with the worse vision, with the second eye to follow, typically within a month. Same-day surgery for both eyes is avoided to prevent bilateral complications such as infection.
Phacoemulsification remains the preferred surgical method in the developed countries, but in recent years manual small incision cataract surgery (SICS) has gained acceptance, especially in most developing countries. A meta-analysis comprising of 76,838 eyes compared the safety and efficacy of SICS compared to the traditional phacoemulsification. The meta-analysis revealed no differences between phacoemulsification and SICS for best-corrected visual acuity and uncorrected distance visual acuity. The average procedural time for SICS is lower than phacoemulsification and the cost is less than half because SICS requires less equipment.(11) Therefore, SICS is a better option for underserved areas with a large population backlog waiting for surgery.
After cataract surgeries, the patients may notice immediate vision improvement. Operative and post-operative complications for cataracts are uncommon. The most significant complications include infections and bleeding, which occur in less than 1% of all cataract surgeries performed. However, in the risk-prone population, such as high myopia and post-trauma eyes, the rates may be much higher. The recovery period for cataract surgery is typically within one to two weeks, although some patients may require longer time to recover if an underlying condition, such as diabetes, is present.
A database study investigated trends in outcomes of cataract surgery in patients who had undergone cataract extraction in the Netherlands, Sweden, or Malaysia from 2008 through 2012. The 5-year trend in all three national data sets showed decreasing visual thresholds for surgery, decreasing surgical complication rates, and increasing visual outcomes regardless of the initial preoperative visual level.(7)
Implanted intraocular lenses will last the life of the patient in most cases. Posterior capsule clouding may form months to years after a cataract surgery. Posterior capsule opacification is the most common complication after cataract surgery, with an incidence of 30%.(12) The opacifications cause vision decline and will need to be removed by a special laser; the procedure is called ND:YAG (a crystal that is used as a lasing medium for solid-state lasers) laser posterior capsulotomy. This procedure is considered routine post-surgery, and only takes minutes to perform, without returning to the operating room.
Surgical Intraocular Lens Choices
Monofocal lens: The standard lens choice for the vast majority of patients is the monofocal lens, which allows a preset focal point for distance, intermediate, or near vision. For instance, with a distance monofocal lens implanted, another pair of reading glasses would be needed to read. This class of lenses is covered by insurance and Medicare.
Toric lens: This lens choice is for patients with significant astigmatism. Implantation of this lens removes the distortion associated with astigmatism and is highly accepted by physicians and patients. This class of lenses is generally not covered by insurance and Medicare.
Multifocal lens: This lens choice allows a range of clear vision for both distance and near, which may obviate the need for glasses. However, a certain patient population may experience visual distortions with this lens, resulting in a need for lens-exchange surgery after the initial cataract surgery. This class of lenses is generally not covered by insurance and Medicare.
Accommodating lens: This lens choice allows changes in focal point with shifting position of lens hinges. Certain patients may also experience visual distortions with this lens. This class of lenses is generally not covered by insurance and Medicare.
Monovision: This monofocal lens choice is uncommon but for certain patient population offers the ability to avoid wearing glasses post-operatively. The dominant eye is usually set with a monofocal lens for distance vision, while the non-dominant eye is set for near vision. This class of lenses is covered by insurance and Medicare.
New Treatment on the Horizon
Surgical treatment is very effective and safe for cataracts. However, it requires specialized equipment and highly trained physicians unavailable in most underserved areas of the world.
In recent cataract research, several new studies have investigated peptide-based treatment strategies for cataract that has the potential to medically slow down disease progression.(13)(14)(15) Because cataract formation is attributed to insolubility and aggregation of proteins in an aging eye, it is possible to identify specific peptide that could block protein aggregation, which in turn delay cataract formation or break up already formed cataracts. Screening of small molecules that inhibit protein aggregation will allow a preclinical study that may reveal new targets for cataract formation; these peptides could be packaged as drugs and used to not only prevent aggregation but also to enhance disaggregation of formed cataract.
In conclusion, age-related cataract formation is a common and treatable condition. Cataract surgery is a highly successful procedure for patients suffering with visually significant disease. Future research may provide medical therapeutics that can slow down the progression of the disease.