Course Authors
Ashish R. Panchal, M.D., Ph.D., R.D.M.S., Creagh Boulger, M.D., Amar Vira, M.D., and David Bahner M.D., R.D.M.S.
Dr. Panchal is Assistant Professor of Emergency Medicine and Director of the Center for EMS; Dr. Boulger is Assistant Professor of Emergency Medicine and Associate Director of Ultrasound; Dr. Vira is Ultrasound Fellow; and Dr. Bahner is Professor of Emergency Medicine and Director of Ultrasound, Ohio State University Wexner Medical Center, Columbus, OH .
Within the past 12 months, Drs. Panchal, Boulger, Vira and Bahner report no commercial conflict of interest.
Albert Einstein College of Medicine, CCME staff, and interMDnet staff have nothing to disclose.

Albert Einstein College of Medicine – Montefiore Medical Center designates this enduring material activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
In support of improving patient care, this activity has been planned and implemented by Albert Einstein College of Medicine-Montefiore Medical Center and InterMDnet. Albert Einstein College of Medicine – Montefiore Medical Center is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
Upon completion of this Cyberounds®, you should be able to:
Articulate the key events and documents that have led to the current culture of focused ultrasound use in North American emergency medicine;
Apply the current use of focused ultrasound in the emergency department to assist with medical decision-making;
Highlight the necessary components that will affect the future of focused ultrasound in the emergency department and throughout the health care system.
Emergency Medicine (EM) became the 24th board of the American Board of Medical Specialties (ABMS) in 1978.(1) Since then, the annual number of patient emergency department (ED) visits has steadily increased and now exceeds 100 million per year in the United States alone.(2) Adding to this challenge is an associated rise in patient complexity, which has dramatically increased the need for diagnostic bedside imaging to serve these patients. It is now estimated that emergency medicine physicians and trainees use ultrasound in over 92% of academic emergency medicine departments in the United States.(3)
Focused ultrasound (point of care) is defined as the act of bringing ultrasound (US) evaluation to the bedside for real-time performance.(4) Since these US images are collected immediately by the practitioner, they directly guide the physician's medical decision-making process.
The use of focused ultrasound in EM has significantly improved patient care. In this Cyberounds®, we will: (1) describe the development of emergency ultrasound; (2) describe the current uses of focused ultrasound in EM with emphasis on specific core areas; and (3) discuss future areas of innovation including education, venues of use and administration.
Development of Emergency Ultrasound
The expansion of bedside ultrasound occurred as a consequence of a professional policy initiative by the American College of Emergency Physicians (ACEP) in 1990. ACEP declared that ultrasound should be available for all emergency department patients. To facilitate the development of emergency ultrasound to this ideal, by 1994, Dr. James Mateer and others had created a "model" curriculum for ultrasound in emergency medicine.(5)
Though debates continued between 1994 and 1999 with regard to the appropriate use of ultrasound by emergency practitioners, training programs and fellowships in the technology slowly developed. In 1999, the American Medical Association decided in House Resolution 802 that each specialty had to determine their own scope of practice and each provider had to apply for privileging at the local credentialing committee of the hospital facility.(6) This allowed that focused ultrasound could be used by all specialties according to their training guidelines and that they would not have to adhere to the guidelines of traditional imaging specialties.
Emergency medicine resident training in the 21st century now typically includes the use of focused ultrasound and can continue training through ultrasound fellowships. The ACEP developed (2001) guidelines for the initial scope of practice that outlined training topics, methods, assessment and criteria for ultrasound privileging.(7) The topics initially codified focused US training for emergency medicine into seven key areas: cardiac, abdominal aorta, trauma, procedural, renal, pelvic and hepatobiliary. Four additional indications were added (2008): musculoskeletal (MSK), thoracic, vascular and ocular ultrasound (Table 1).(8)

Table 1. Areas of Focused Ultrasound Training As Described by the ACEP Policy Statement.(8)
| Cardiac: assessment of contractility and pericardial fluid |
| Abdominal aorta: presence of AAA |
| Trauma: detection of abnormal fluid or air collection in the torso |
| Procedural: for guidance of a needle for procedures such as vascular access |
| Urinary tract: detection of the presence of hydronephrosis and bladder status |
| Intrauterine pregnancy: determination of an intrauterine pregnancy |
| Hepatobiliary: determine biliary inflammation and biliary obstruction |
| Soft Tissue/Musculoskeletal: abscess and foreign body identification, detect tendon injuries and joint effusions |
| Thoracic: determine presence of pneumothorax or fluid |
| Vascular: determine the presence of DVT |
| Ocular: detect retinal detachment/vitreous hemorrhage |
Current Practice of Ultrasound in Emergency Medicine
The practice of focused ultrasound in EM is directed toward the key ACEP topics noted in Table 1. Each of these has a significant impact on patient throughput and outcomes. In this Cyberounds®, we will focus on specific areas of focused US in EM that are most frequently utilized by practitioners including: cardiac assessment, volume assessment, abdominal aorta evaluation, trauma evaluation — FAST scan, procedural guidance, pelvic ultrasound for first trimester pregnancy, and thoracic ultrasound for pneumothorax.
Cardiac Ultrasound
The ED assessment of cardiac activity and function has become an important part of emergency practice. Bedside echocardiography may be used in many life-threatening scenarios and is able to provide real-time data for the management of clinically unstable patients such as those who present with chest pain, shortness of breath, hypotension or cardiac arrest.(9) Several important algorithms for assessment of hypotension (e.g., RUSH, FAST, EFAST) include cardiac evaluation as an important component.(10)(11)
Within the specific scope of practice for emergency physicians is the assessment of cardiac function, detection of pericardial effusions and evaluation of right heart strain.(9) To obtain cardiac US views can be challenging. The four key views commonly assessed include subxiphoid, parasternal long axis, parasternal short axis and the apical 4-chamber view (Figure 1-4). Utilizing these acquired views, the physician can accurately assess cardiac activity, left ventricular function and right heart strain.(12)(13)
Figure 1. Image for Sonographic Evaluation of the Heart.
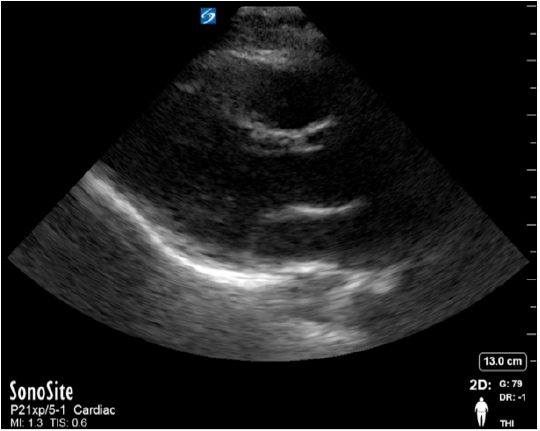
Parasternal long axis view of the heart.
??f
Figure 2. Image for Sonographic Evaluation of the Heart.
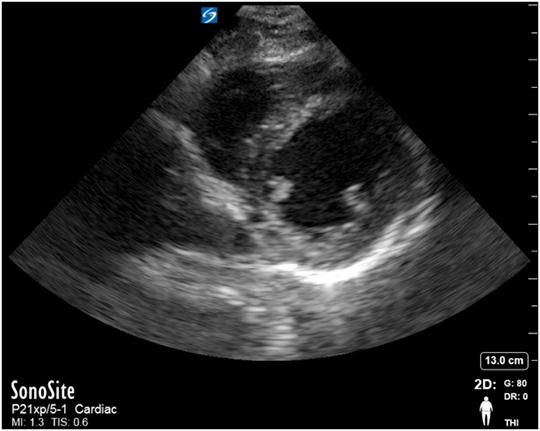
Parasternal short axis view of the heart.
Figure 3. Image for Sonographic Evaluation of the Heart.
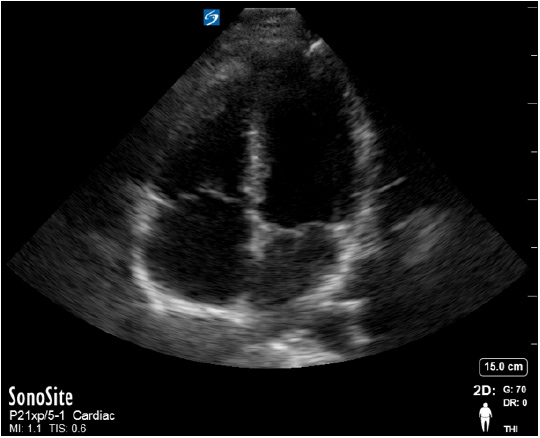
The image is the apical 4-chamber view. Abbreviations: RV, right ventricle; LV, left ventricle; RA, right atrium; LA, left atrium.
Figure 4. Image for Sonographic Evaluation of the Heart.
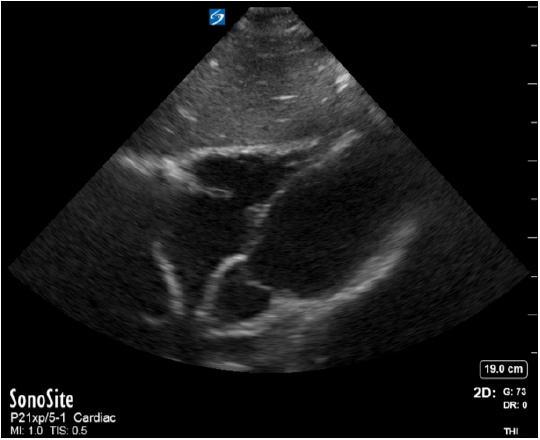
Subxiphoid view of the heart. Abbreviations: IVS, intraventricular septum; L, liver; LA, left atrium; LV, left ventricle; MV; mitral valve; RA, right atrium; RV, right ventricle.
Volume Assessment and Fluid Responsiveness
In critically ill patients, the assessment of volume status is an important aspect of resuscitation.(9) Faced with a patient in shock, there is a critical need to differentiate its cause, since treatment with fluids may cause harm to patients with cardiogenic etiologies. Thus, focused sonographic evaluation of volume status and fluid responsiveness in the critically ill patient becomes essential.
Among the US methods to assess volume status and fluid responsiveness, measurement of the inferior vena cava (IVC) for estimates of central venous pressure (CVP) and volume responsiveness is the most commonly used (Figure 5).(14)(15) However, the estimation of volume and its relationship to CVP is limited since it is often unreliable and a poor predictor of responsiveness.
IVC measurement of fluid responsiveness is performed by comparing the diameter of the vessel at both end expiration and respiratory collapse (see Figure 6 below).
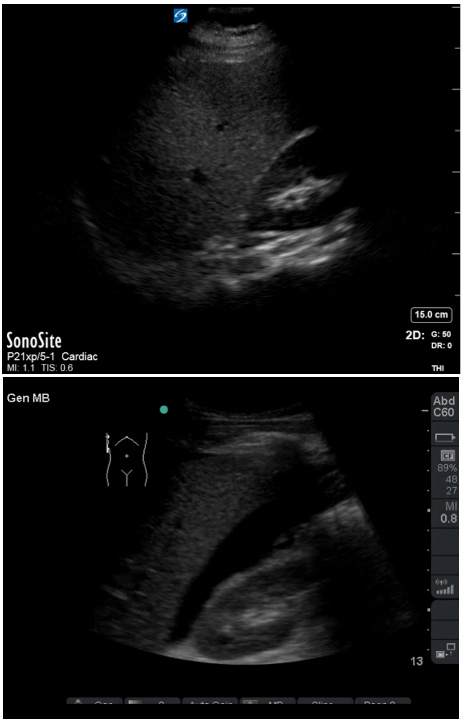
Figure 5. Sonographic Evaluation of the IVC in the Subcostal Window.
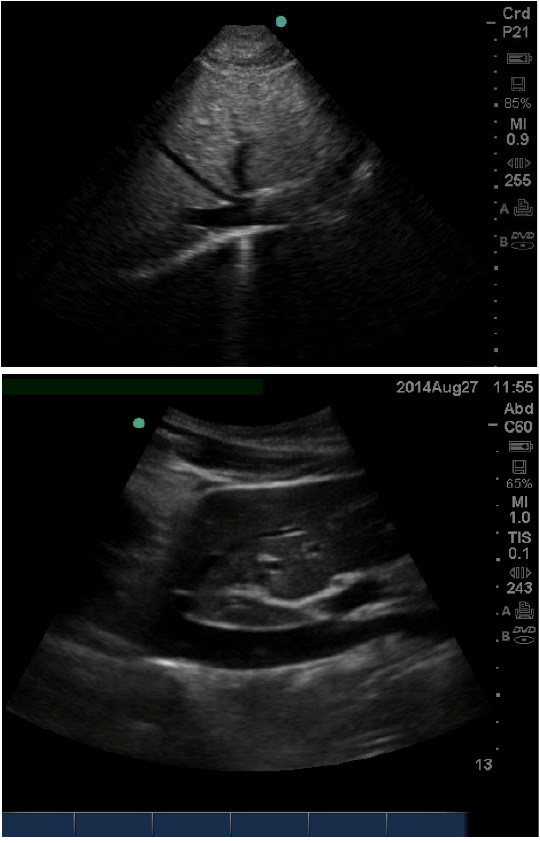
Upper image is subcostal short axis view of the IVC. The IVC is joined by the hepatic veins [right, middle and left hepatic veins (HV)] proximal to the entry to the RA. In the lower, the long axis of the IVC is seen traversing the liver just posterior to the caudate lobe with the hepatic vein draining prior to the right atrium.
The IVC is visualized in the subcostal view and the diameter is measured in the long axis. The location of measurement is prior to the junction of the hepatic veins that are proximal to the entry to the right atrium. Measurement of respiratory collapse is done in non-intubated patients at the same location following a sniffing maneuver by the patient [quick short breath to increase intrathoracic pressure (Figure 6)].
Figure 6. M-Mode Tracing of the IVC Measurement in the Subcostal View at both End Expiration and with Respiratory Collapse.
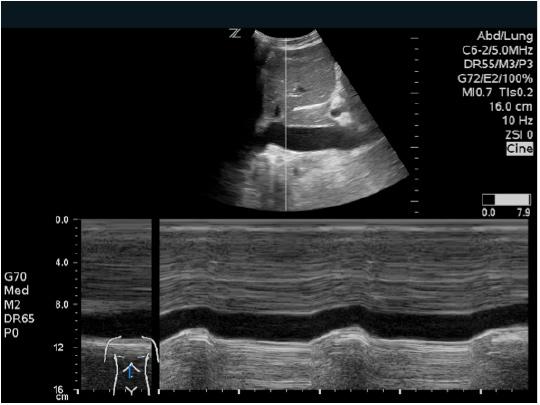
The IVC diameter at respiratory collapse is measured through a sniffing maneuver by the patient as noted in the image. This patient is euvolemic with a diameter between 1.5 and 2 cm with <50% collapse.
The relationship of IVC diameter, respiratory collapse and CVP has been described in detail and is noted in Table 2.(16)
Table 2. Relationship of Inferior Vena Cava (IVC) Diameter and Respiratory Collapse to Approximate Central Venous Pressure (CVP).
| IVC Diameter (cm) | Respiratory Collapse with Sniffing (%) | CVP (mm Hg) |
|---|---|---|
| <1.5 cm | >50% | 0-5 mm Hg |
| 1.5-2.5 cm | >50% | 5-10 mm Hg |
| 1.5-2.5 cm | <50% | 10-15 mm Hg |
| >2.5 cm | Loss of phasicity | 15-20 mm Hg |
This measurement is most reliable in non-intubated patients and is less accurate in intubated patients due to the effect of positive pressure.(15) However, several studies have demonstrated reliable assessment of fluid responsiveness in mechanically ventilated patients by measuring IVC distention and variability.(17)(18)
Abdominal Aorta
As part of the evaluation of undifferentiated hypotension, one possible etiology in patients >60 years old is a ruptured abdominal aortic aneurysm (AAA). Early diagnosis is critical for survival since the overall mortality from a ruptured AAA exceeds 90%.(19) Sonographic evaluation of an AAA is done using a curvilinear probe starting at the subcostal window, similar to the IVC measurement. The aorta is identified by noting the vertebral body in the transverse view which appears as a hyperechoic arc followed by posterior shadowing. The aorta lies immediately above the vertebral body and normally measures <3 cm (Figure 7).(20)
Figure 7. Transverse View of the Abdominal Aorta.
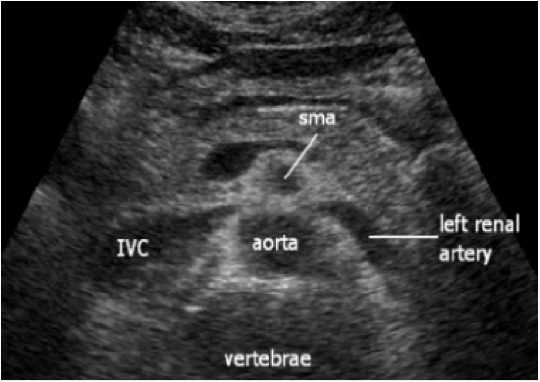
Notice the hyperechoic arc of the vertebral body with posterior shadowing. The abdominal aorta lies immediately above this structure throughout its course in the abdomen caudally.
The aorta's dimensions are then evaluated caudally to the bifurcation into the iliac arteries. Sonographers measure outer wall to outer wall in the transverse view to minimize any underestimations in the longitudinal view (Figure 8).
Figure 8. Abdominal Aortic Aneurysms Evaluated by Focused Bedside Ultrasound.
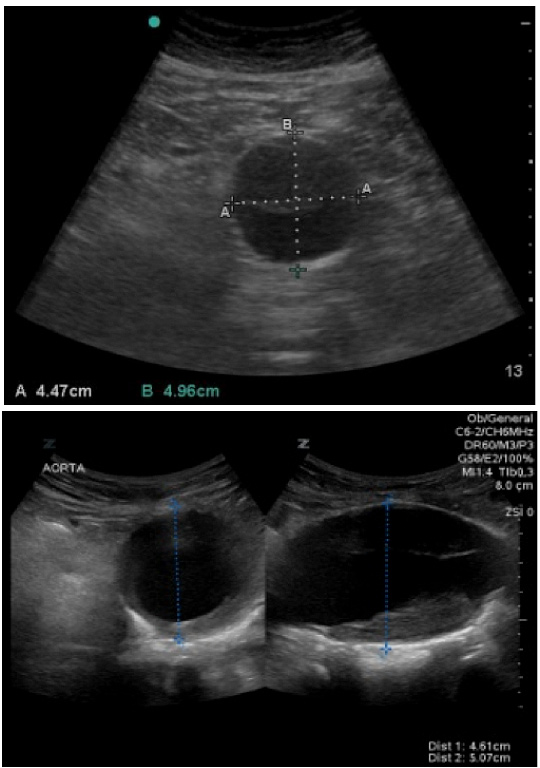
Measurements of an AAA are done in the transverse view (upper and lower images). The longitudinal view allows for imaging the extent of the AAA (lower image).
Imaging of the aorta, as it courses caudally, should also be performed in the longitudinal view where many of the branches of the aorta will be seen more clearly (Figure 8). The challenges of sonographic evaluation of the abdominal aorta are both patient habitus and bowel gas.
If appropriately visualized, real-time focused ultrasound of the aorta is highly sensitive for the presence of AAA.(21) Ultrasound is not able, however, to reliably determine acute AAA rupture or the presence of retroperitoneal hemorrhage.
Trauma Evaluation - FAST Scan
In the emergency department, the determination of whether a hypotensive trauma patient requires immediate transfer to the operating room is a lifesaving decision. This is done using the FAST (focused assessment with sonography in trauma) exam.
(11) The FAST exam, specifically indicated for trauma patients and hypotensive patients, is one of the most widely used, focused ultrasound applications for evaluating the presence of pericardial or peritoneal fluid. With a curvilinear probe, the sonographer searches four windows of the body for the presence of free fluid.(11),(22) The windows include: (1) the perihepatic (evaluating Morison's pouch) (Figure 9); (2) the perisplenic (focusing onFigure 9. FAST Scan: Hepato-renal View.
Upper image demonstrates a normal FAST image. Lower image demonstrates a positive FAST scan with free fluid (black) in the hepatorenal junction.
Figure 10. FAST Scan: Splenorenal View.

Upper image demonstrates a normal captured image of the left upper quadrant evaluation. The lower image is a positive FAST scan with free fluid (black) noted in the spleno-diaphragm interface.
Figure 11. FAST Scan: Pericardial view.
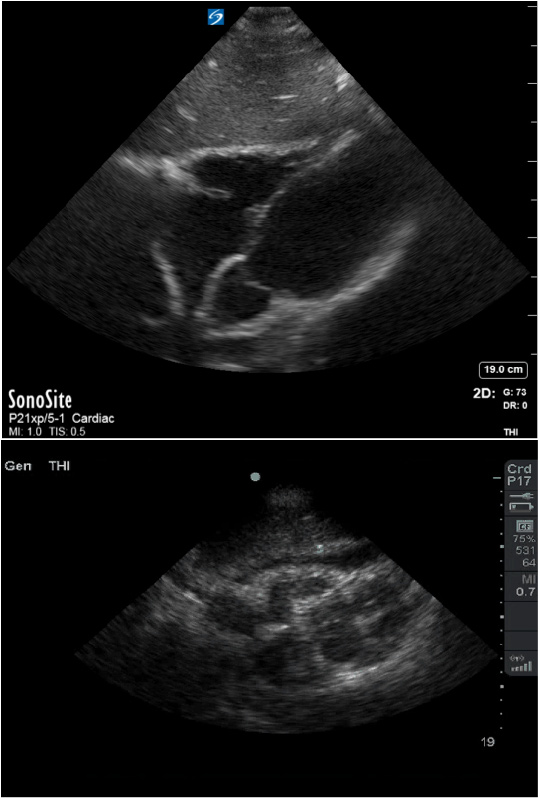
Upper image demonstrates a normal subxiphoid image of the heart using the liver as the sonographic window of evaluation. The lower image demonstrates a positive FAST scan with pericardial free fluid (black) around the heart.
Figure 12. FAST Scan: Pelvic View.
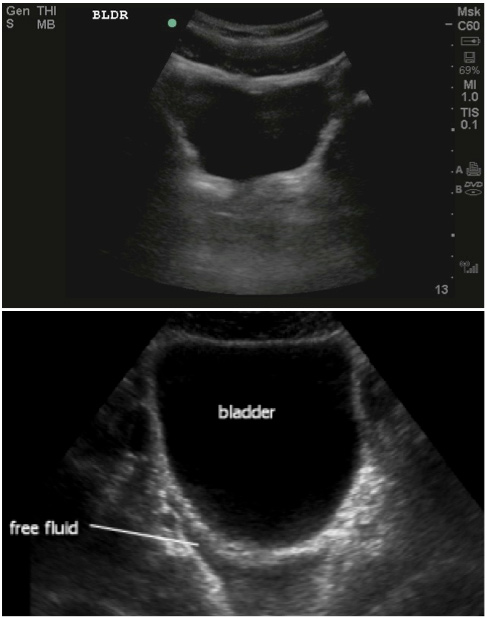
The upper image demonstrated a normal pelvic view of the FAST scan. The lower image demonstrates a positive FAST scan with free fluid below the bladder (black).
The FAST exam has a sensitivity of 60-98% and a specificity of 84-98% but is often operator-dependent.(23)(24)(25) Penetrating trauma, bowel injuries and retroperitoneal bleeding, however, cannot be definitively diagnosed by FAST. Further, because the FAST scan searches for the presence of fluid, evaluation early in the trauma may only reveal minimal bleeding and result in a negative FAST. The FAST can also be misinterpreted as positive in the setting of ascites. Thus, the FAST scan's role is that of a screening test to determine whether a patient, if unstable, needs
Procedural Uses of Ultrasound
The use of focused ultrasound for procedures, compared to other applications of US, has been rapidly integrated into overall clinical practice. Ultrasound guidance is applicable to numerous procedures by many specialties.(4)(26) Its diagnostic popularity is largely due to its significant impact on patient safety.(27) The primary use of focused ultrasound for procedures for many practitioners is vascular access. Ultrasound guidance has been demonstrated to decrease failure rate, number of attempts and procedure complication rates including arterial injury and pneumothorax.(28)(29) The vessel to be cannulated is imaged in both the long axis and short axis views (Figure 13).
Figure 13. Sonographic Evaluation of the Internal Jugular Vein.
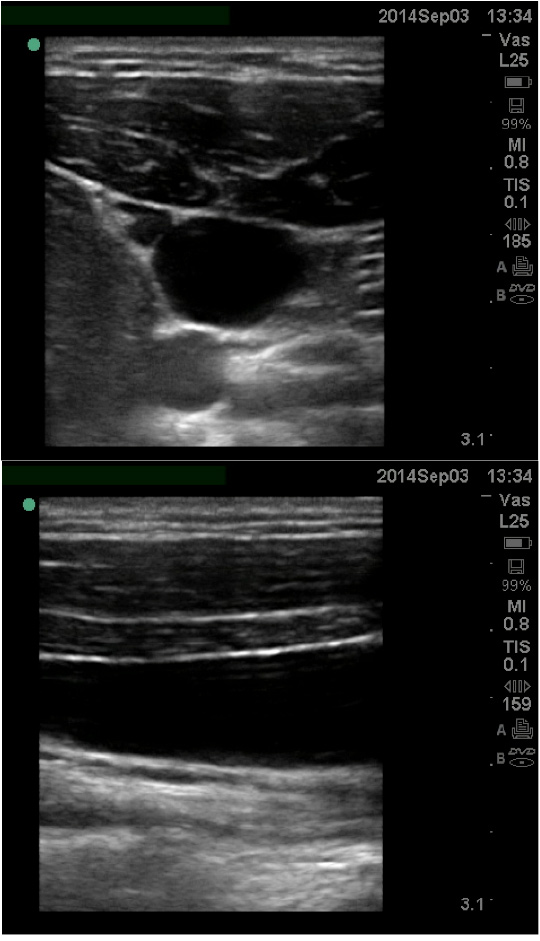
The upper image shows the internal jugular vein and the carotid in the short axis, the lower image shows the internal jugular vein in the long axis with the appearance of a "tube."
The vein is defined by its anatomical location, presence of a thin wall, compressibility, and low flow Doppler waveform on evaluation. In either orientation (i.e., long axis or short axis), the needle tip is visualized from the surface and then guided to the vessel and followed as it enters the vessel (Figure 14).
??fFigure 14. Cannulation of Venous Structure in the Long Axis and the Short Axis.
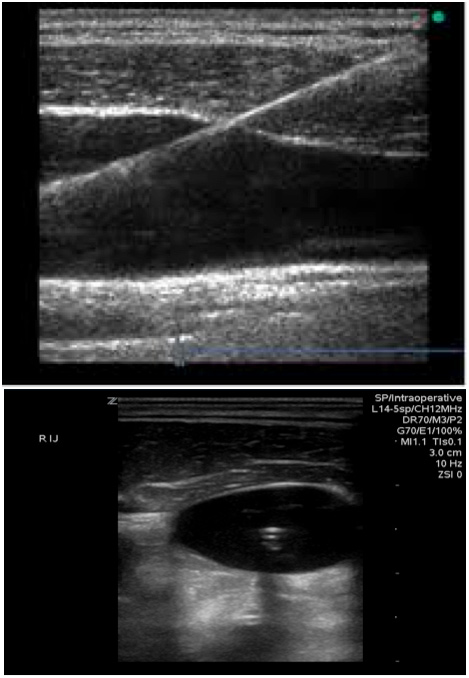
In the long axis (top image), the complete needle length is shown in the field of view. In comparison, in the short axis view (bottom), only the needle tip is noted in the middle of the vessel.
This same technique can be applied to a myriad of procedures in the emergency department including: paracentesis and thoracentesis (Figure 15), joint aspirations (Figure 16), nerve blocks, lumbar puncture and biopsies.(26)
Figure 15. Fluid Collections for Paracentesis and Thoracentesis.
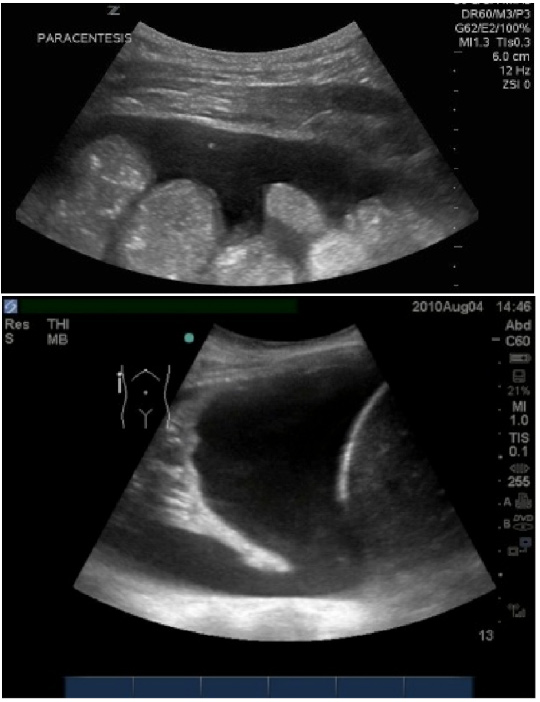
The upper image demonstrates a paracentesis with the needle in the pocket of fluid. The lower image demonstrates a pleural effusion imaged prior to thoracentesis.
Figure 16. Sonographic Images of a Joint Aspiration.
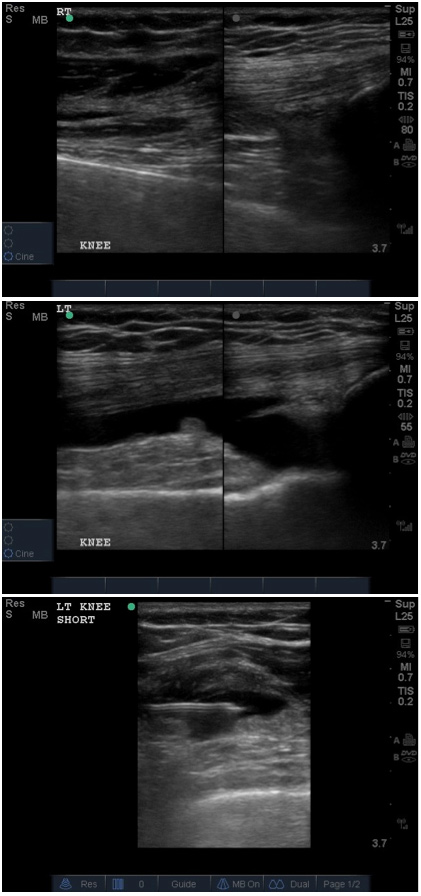
The top image demonstrates a normal knee joint without effusion; the middle image (right) demonstrates an effusion; the bottom showed a needle aspiration of joint effusion.
Pelvic Ultrasound for First Trimester Pregnancy
Point of care pelvic ultrasound has become a valuable tool for bedside practitioners, especially for the expedited evaluation of patients with abdominal pain or vaginal bleeding in the first trimester of pregnancy.(30) The primary concern for these patients is the presence of ectopic pregnancy, which has been found to be as high as 13% in symptomatic ED patients.(31)(32)
A recent meta-analysis demonstrated that emergency physicians are able to accurately identify patients at risk for ectopic pregnancy through the use of bedside focused ultrasound.(33) Early pelvic ultrasound, to rule in the presence of an intrauterine pregnancy (IUP), enables the practitioner to rule out ectopic pregnancy, with a negative predictive value nearing 100% when patients have had no reproductive assistance.(8)
Based on the gestational age, the ultrasound of the pregnant patient's uterus can be done either transabdominally utilizing a curvilinear probe or transvaginally with an endoluminal probe. The transabdominal evaluation is performed by imaging through the suprapubic window similar to the pelvic view of the FAST scan (Figure 17). Optimally done with a full bladder used as a sonographic window, the uterus is imaged in the short and long axes. An intrauterine pregnancy is confirmed by the presence of a gestational sac with a yolk sac, fetal pole or heart activity.
Figure 17. Transabdominal Long Axis Image of an Intrauterine Pregnancy.

Notice the use of the full bladder as the sonographic window for imaging the uterus.
The transvaginal ultrasound (TVUS) evaluation is obtained via the vaginal vault using an endoluminal probe. This route allows for direct ultrasound visualization of the cervix, posterior cul-de-sac and uterus, and can confirm pregnancy at earlier gestational ages. Evaluations of the long and short axes are conducted to confirm the pregnancy (Figure 18). The typical "discriminatory zone" where an IUP should be demonstrated on TVUS is a beta-HCG of 1500- 3000.(34)
Figure 18. Uterus and An Intrauterine Pregnancy Through Transvaginal Imaging.
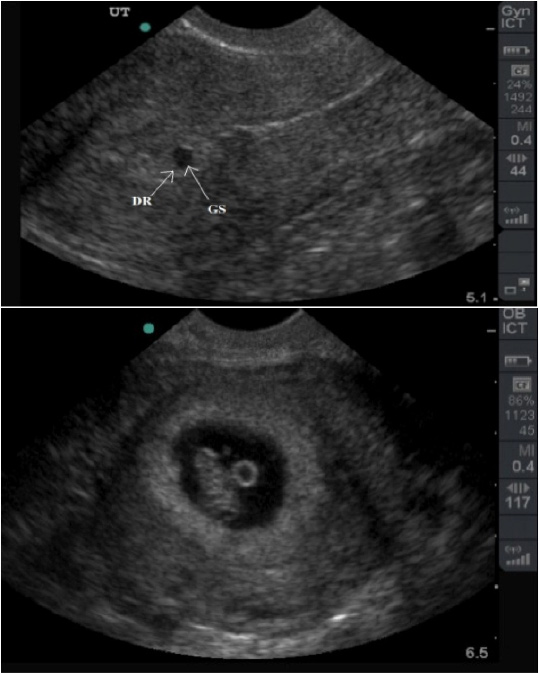
Upper image is a long axis view of the uterus with a gestational sac (GS) and decidual reaction (DR) with no clear intrauterine pregnancy. An intrauterine pregnancy is confirmed in the lower image with visualization in short axis of a gestational sac, fetal pole and yolk sac.
Following confirmation of an intrauterine pregnancy through transabdominal or transvaginal US, the focused evaluation is then directed at measuring fetal heart rate by placement of an M-mode (motion mode) trace line through the visualized heart (Figure 19).
Figure 19. Transvaginal Imaging of An Intrauterine Pregnancy with Measurement of Fetal Cardiac Activity.
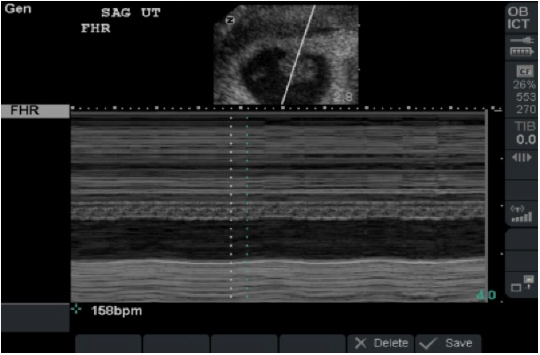
Heart rate is measured through a M-mode trace through the visualized heart and monitoring cardiac pulsations as noted above.
Thoracic Ultrasound
The lung was once considered unsuitable for ultrasound evaluation because it is filled with air, which tends to provide poor sonographic windows. But rapidly evolving technology has now made thoracic ultrasound a useful point of care technique. Pathology such as pneumothorax, interstitial edema, pleural effusion, hemothorax, pneumonia and atelectasis can all be detected with point of care ultrasound.(35)(36)(37)
Currently, the most common use of focused thoracic ultrasound is the evaluation of pneumothorax. Thoracic ultrasound has been shown to be more accurate in detecting pneumothorax than chest x-ray and auscultation. Standard supine chest radiography inconsistently detects pneumothorax, with sensitivities ranging between 50% and 90%.(38)(39)(40) In contrast, according to a recent study, bedside ultrasound was 90.2% sensitive and 98.8% specific for the detection of pneumothorax.(41)
Evaluation of pneumothorax is achieved through visualization of the anterior chest wall using a curvilinear or linear probe (Figure 20). The image generated demonstrates the ribs with the pleural line below. The movement of the lung along this pleural line (lung sliding) determines the presence or absence of a pneumothorax (Figure 20). This is confirmed by placing an M-mode tracing on this area and looking for movement of the pleura (Figure 21).
Figure 20. Imaging of the Thorax by Focused Bedside Ultrasound.
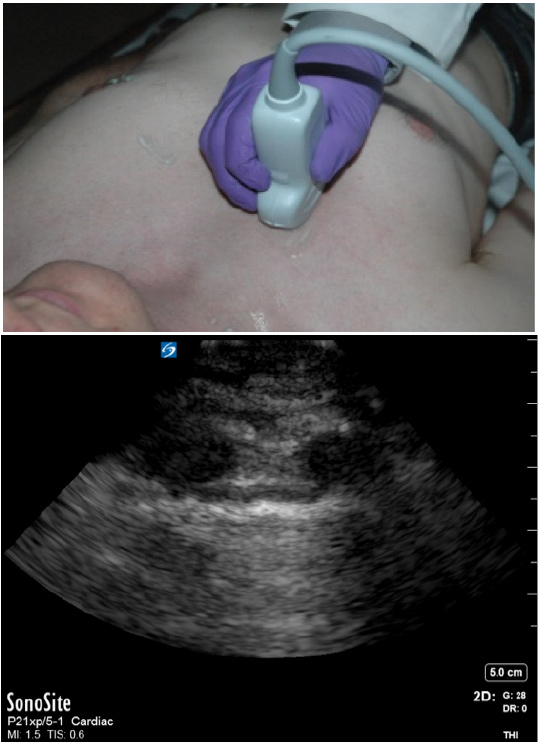
This can be done using the curvilinear probe (upper). The generated image demonstrates the ribs with the pleural line below. Movement of this pleural line with breathing is evaluated for the presence or absence of pneumothorax.
Figure 21. Transthoracic Evaluation With A Curvilinear Probe for Pneumothorax.
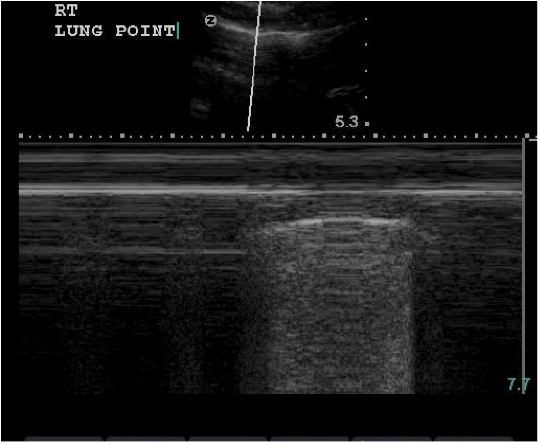
An M-mode trace demonstrates the presence of a pneumothorax and the "lung point" where there is normal lung sliding.
Future Practice of Ultrasound in Emergency Medicine
The use of focused bedside ultrasound in emergency medicine has grown dramatically. The areas of current practice described above are only a few of the many applications of focused ultrasound for clinical practice.8 Because of the growing awareness of the increased risk of malignancy from radiation exposure secondary to serial computer tomography studies (i.e., CAT scans) and a greater emphasis on ALARA ("as low as reasonably achievable"), the use of ultrasound as a safe alternative is becoming even more attractive.(42) As emergency physicians confront more clinically challenging patients, the real-time bedside diagnostic ability of ultrasound becomes a key tool for the management of critically ill patients.(4)(8)
Due to this movement toward increased non-invasive technology, there are three specific areas of expected innovation: education, venues of use and administration.
Education
Bedside focused ultrasound development is driven by the improvement in technology with optimization of the ultrasound machine capabilities and resolution. The technological advances have, however, outpaced professional education. As future practitioners assess their "black bag" of diagnostic devices, ultrasound may be a common diagnostic tool of assistance to invasive procedures and possibly therapeutic interventions. As a result, the skills of focused ultrasonography will need to be integrated into the educational process so future physicians can stay apace of this steady innovation.
Future training of practitioners should begin early in the medical education process during medical school.(43)(44)(45) Improved collaboration and coordination among the accrediting organizations will be needed. US can be learned and mastered if training is started early in medical school anatomy and physiology classes, and subsequently reinforced through simulation opportunities and standardized assessment such as objective structured clinical examinations (OSCEs).
Coordination between undergraduate medical education (UME) and graduate medical education (GME) will be needed. This could include a basic core competency such as vascular access for all medical students. As students separate into their eventual specialty fields during their clinical years, advanced competencies could be created to prepare them for using ultrasound in their future practice.
Venues of Use
The technological advances that have improved the performance of ultrasound machines have further allowed for the expansion of the applicable footprint of the device. As the technology increasingly miniaturizes, US utilization within and outside the hospital setting will expand. The World Health Organization projects that radiography and ultrasound, whether combined or separate, will satisfy two-thirds of all imaging needs in the developing world.(46) And ultrasound in austere environments such as mountainous, jungle, or outer space settings, already a capability, could further increase its impact on health care beyond the hospital setting.(47)(48)(49)(50)
As the technology migrates to smartphones, smart devices, or even wearable technology, the impact of this safe modality to image the body could benefit many seeking health care, as well as answers to their clinical problems.
Administration
As more clinical specialties begin to incorporate ultrasound training into their residency and fellowships, ultrasound use will continue to grow. EM practitioners have become experienced in this relatively new concept of focused ultrasound at the bedside. Their experience in the documentation, saving images, billing and credentialing in ultrasound can help other specialties integrate ultrasound into their practice.
The rapid development of ultrasound does, however, set the stage for possible dangers in clinical practice. With the increased utility and accessibility of this technology, combined with the fact that it is a user-dependent technology, care must be taken to ensure appropriate training and quality assurance of practitioners. Indiscriminant use without oversight may lead to increased medical errors and unnecessary confirmatory testing due to false positives. This would increase the burden on the health care system and jeopardize optimal patient care.
Continued evaluations of focused ultrasound algorithms to optimize care and confirm patient-centered performance will also be necessary. Rigorous research studies to evaluate outcome measures of focused ultrasound, with emphasis on the comparison of its performance to the current standard of care both in clinical accuracy and cost effectiveness, will be integral to the development of valid algorithms.
Conclusions
The future of clinical ultrasound is bright as the devices continue to improve their capabilities and resolution. Future use of ultrasound in the clinical setting may be enhanced as diagnostic algorithms evolve to account for the high cost of care and the inefficiency that characterizes the current health care system. The full integration of ultrasound into the medical education paradigm is still years away, yet the rise in ultrasound usage, begun by emergency medicine practitioners advocating and codifying the concept of focused clinician-performed ultrasound, will likely dominate 21st century medicine.