Course Authors
Youhua Zhang, M.D., Ph.D., and Todor N. Mazgalev, Ph.D.
Release Date: 08/16/2010
Upon completion of this Cyberounds®, you should be able to:
Discuss the current status of efforts to control the atrial fibrillation epidemic
Describe the rhythm versus rate control approaches
Discuss the intracardiac autonomic nervous system, and specifically the selective vagal control of atrioventricular nodal conduction.
Discuss state-of-the-art new technologies utilizing implantable neural electrostimulators to achieve selective modulation of the intracardiac autonomic nervous system in order to control AV conduction and ventricular rate during atrial fibrillation.
Assess critically different therapeutic options, including the latest application of implantable neural electrostimulators.
Introduction
Atrial fibrillation (AF) is the most common clinically significant cardiac arrhythmia, with an estimated 2.3 million Americans having AF.(1)(2)(3) The prevalence of AF increases with age, reaching about 9% for those older than 80.(1)(4) Due to the aging of population, the number of AF patients is estimated to increase 2.5 times during the next 50 years.(1)(3) AF accounted for approximately one-third of all hospitalizations with a cardiac rhythm disturbance,(4)(5) and significantly increased the risk of ischemic stroke two to seven times among patients with nonrheumatic heart disease, and up to 17 times in patients with rheumatic heart disease.(6) The total mortality rate is approximately doubled in patients with AF compared with patients in normal sinus rhythm(7)(8)(9).
Electrophysiologically, AF is characterized by a rapid and irregular activation of the atria, typically at 400 to 600 beats per minute (bpm) in humans. At such non-physiologically high rates, the atria lose their pumping function. Instead of contracting, the atria are only quivering. Thus, the hemodynamic contribution from a coordinated atrial contraction is lost. During AF, the ventricular rate is no longer under physiological control of the sinus node; instead it is determined by interactions between the atrial electrical activations and the filtering function of the atrioventricular (AV) node. The latter is the only normal structure responsible for the conduction of atrial impulses to the ventricles.
Despite the life saving role of the AV node in filtering these rapid atrial firings, without proper treatment AF normally results in a rapid, irregular ventricular rate. These rapid, irregular beats can cause many symptoms such as palpitation, chest discomfort, light-headedness and syncope. Furthermore, the loss of atrial contractions increases thromboembolic risk due to blood stasis in the fibrillating atria leading to clot formation.(15) The long-term tachycardia from uncontrolled ventricular response could lead to tachycardia-induced cardiomyopathy.(10)(11)(12) In fact, AF remains one of the leading causes of clinical deterioration in heart failure patients.(13) Thus, a proper rhythm control (restoration and maintenance of normal sinus rhythm) or ventricular rate control (maintenance of an optimal ventricular rate) become essential to avoid development of severe heart failure.(14)
"Rhythm Control" Versus "Rate Control"
Currently there are two broad strategic treatment options for AF treatment: rhythm control and rate control. For rhythm control, the treatment is directed toward restoring and maintaining the normal sinus rhythm; for rate control, therapies are used to slow ventricular rate to a hemodynamically optimal level, while allowing AF to persist. In those patients with continuous AF, anticoagulation is necessary due to increased thromboembolic risk.(16)
Theoretically, rhythm control has many advantages over ventricular rate control in AF patients. By providing normal sinus rate and restoring atrial transport function, rhythm control can improve hemodynamics, reduce thromboembolic risks and improve quality of life. However, currently available clinical trials have demonstrated that rate control is as good as rhythm control in terms of reducing morbidity and mortality in patients with AF, even in patients with heart failure.(17)(18)(19)(20)
There are several reasons that could explain why the current rhythm control strategy is not superior to the rate control approach. First, currently there are no available drugs that are fully effective in maintaining sinus rhythm. Antiarrhythmic medications have only limited efficacy for preventing AF recurrence. One-year success rate in maintaining sinus rhythm is only 50-65% despite the best treatment,(21)(22) and is less than 40% after two years.(19) Accordingly, many patients being treated primarily for rhythm control have to switch to rate control because of AF recurrence. Second, during rhythm control treatment, both symptomatic and asymptomatic AF recurrence may increase thromboembolic risk in patients without anticoagulant drugs. Third, all rhythm-control medications have potential serious side effects, including life threatening pro-arrhythmic effects. In the case of the commonly used drug amiodarone, there are other serious side effects such as pulmonary fibrosis, thyroid dysfunction and hepatic toxicity. In addition, many AF patients are considered unsuitable for rhythm control simply because their sinus rate cannot be restored and maintained. Therefore, ventricular rate control and anticoagulation therapy remain the only choice in a majority of AF patients.
A Need for Novel and Effective Therapies
As discussed above, the ventricular rate during AF is determined by the filtering role of the AV node. Thus, all rate control approaches essentially aim to inhibit the AV node conduction, as we have summarized in a previous review.(23) Currently medications (such as β-blockers, calcium-channel antagonists and digitalis) are still the most commonly used therapy in clinical rate control during AF. However, medications are only partially effective and may not be well tolerated in some patients as a consequence of side effects.
When medications have failed to achieve rate control or are not well tolerated due to side effects, other strategies can be considered. For example, the AV node conduction property can be impaired by anatomic modification (such as radiofrequency AV node modification) to achieve rate control for patients refractory to medications. However, the radiofrequency AV node modification is only partially effective and may inadvertently result in permanent AV block that would necessitate lifetime pacemaker therapy. The AV node ablation with pacemaker implantation is the last resort in patients whose ventricular rate control cannot be achieved by other treatments. This approach has the obvious disadvantage of lifetime pacemaker dependency. In addition, there are hemodynamic drawbacks and increased risk of sudden death due to abnormal retrograde ventricular activation sequence after pacemaker implantation.(25)(26) In general, the AV nodal modification should be attempted for AF patients only when nodal ablation with subsequent pacemaker implantation is intended for other concomitant reasons.24
Cardiac resynchronization therapy with biventricular pacing may alleviate some of the above described drawbacks and improve the outcome, although large-scale randomized trials are needed to confirm the benefits.(27) Another ablation approach, with lesions encircling rather than destroying the AV node, has shown to result in acceptable junctional escape rhythm, thus avoiding pacemaker implantation.(28) However, the technique needs further refinements and verification.
As a result of the limitations of currently available treatment options, new and more effective therapies are still needed for ventricular rate control during AF. During the last decade, selective cardiac vagal neuromodulation, which utilizes electrical stimulation to enhance the physiological autonomic control to the AV node, has emerged as a novel beneficial therapy for ventricular rate control during AF.(29)(30)(31)(32)(33)(34)(35)
Selective Cardiac Vagal Neurostimulation: Anatomic and Functional Basis
The AV node area, which is richly supplied with vagal nerves,(36) has a very selective innervation by vagal fibers projecting from postganglionic neurons located in a discrete epicardial fat pad at the junction between the inferior vena cava and the left atrium, near the crux of the heart (Figure 1).(37)(38)(39)(40)

Figure 1. Anatomical Location Of The Atrioventricular Node Fat Pad.
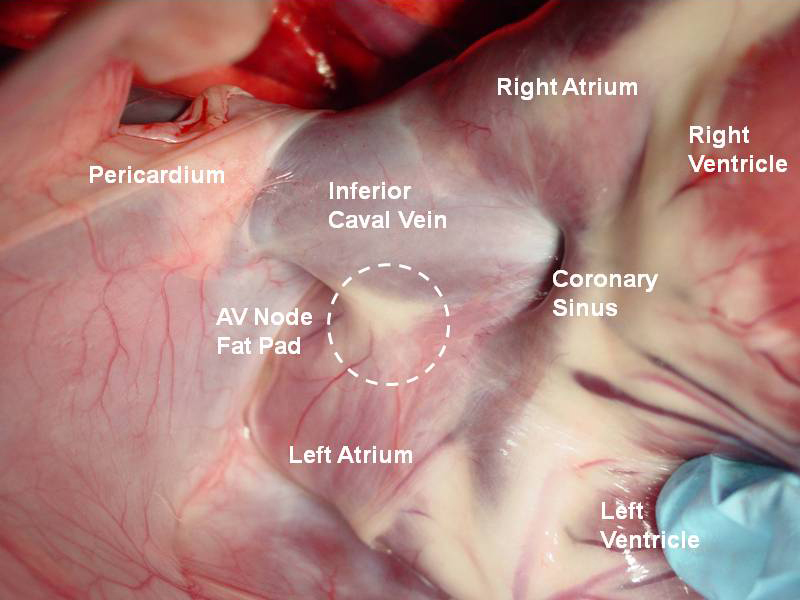
Click image for larger view.
The diagram uses as a background a real anatomical epicardial image of dog heart. The heart has been lifted up toward the head to show the anatomical position of the epicardial AV node fat pad (dashed circle).
When electrical stimulation is applied to this fat pad in the dog heart, the AV nodal conduction is delayed or even fully blocked, while the spontaneous sinus cycle length remains unchanged.(29) A similar fat pad has been identified in patients as well. In 2002, Quan et al.(41) identified a functional human epicardial AV node fat pad in seven patients undergoing coronary artery bypass surgery. Electrical stimulation of this structure (impulse duration 0.10-0.15 ms, frequency of 20-50 Hz, and current strength of 40 mA) produced complete AV block with no change in the sinus rate. It has been noticed that the fat pad also innervates the surrounding right atrium to a distance within 2 cm, judged by atrial effective refractory period changes. No significant change in atrial refractoriness occurred at distances >2 cm. Thus, this study for the first time provided identification of a functional human AV node fat pad.
Due to the fact that vagal nerve projections from postganglionic neurons in the fat pad end selectively within the AV node, this fat pad is frequently referred to as "AV node fat pad." Other names are also used in the literature to identify its anatomical location such as "right inferior ganglionated plexus" or "inferior vena cava-left atrium fat pad." Based on this unique anatomical arrangement of the cardiac vagal network, selective AV node vagal stimulation is possible and has been shown to be effective in slowing ventricular rate during AF.(29)(30)(31)(32)
The physiological basis for such therapy is that electrical vagal nerve stimulation (VNS) and the release of the neurotransmitter acetylcholine (Ach) elicit negative dromotropic effect (that is, slowing) on the AV node conduction. Ach, through the muscarinic M2 receptor-mediated G-protein pathways, activates the acetylcholine-activated potassium membrane current IkACh and reduces slow inward current. As a result, Ach hyperpolarizes the resting membrane potential, inhibits the action potential phase zero upstroke and phase 4 depolarization and reduces the space constant (distance) for electrotonic current spread in the AVN.(42) Mazgalev et al.(43) have documented in isolated rabbit AV node preparations that sub-threshold postganglionic vagal stimulation (PGVS), applied directly onto the endocardial surface above the AV node, produces transient hyperpolarization and subsequent depression of AV conduction. PGVS caused reproducible disorganization of the prevailing excitation wavefront. This was manifested as local nonuniform depression of conduction, action potential hump formations, and alteration in the sequence of depolarization.(44) Depending on the intensity, VNS can prolong the AV conduction time or ultimately produce full AV block.(29)(45)
The vagally induced negative dromotropic effect can be evoked by electrical stimulation applied at different points along the vagal pathways going to the AV node. For example, electrical stimulation delivered to the cervical vagus nerve,(46) intravascular neurostimulation with catheters placed in the superior vena cava,(47)(48) the coronary sinus,(47)(48) the inferior vena cava(49) or the pulmonary artery,(47)(50) as well as epicardial(32)(51)(52) or endocardial(34)(53)(54)(55)(56) ganglionic vagal stimulation, have been demonstrated to be effective in slowing ventricular rate during AF. However, there are different concerns associated with each of the above VNS approaches. Cervical VNS has the potential of broad systemic side effects, even though successful veterinarian use of cervical VNS with an implanted device to control ventricular rate for more than nine months has been reported in a dog with AF.(57) There is an apparent positioning stability issue associated with circular catheters or basket catheters placed inside large vessels, along with concerns for thrombus formation and requirements for high stimulation energy. Currently selective AV node vagal modification for ventricular rate control during AF is predominantly achieved through endocardial or epicardial ganglionic electrical stimulation.
Selective AV node vagal stimulation through the epicardial approach has the advantage of easy electrode placement (see Figure 1) but requires thoracotomy, limiting the application to postoperative AF patients.(51) The endocardial approach, while avoiding the thoracotomy, is more technically demanding to locate the desired stimulation site (see Figure 2) and has the (limited) risks of lead dislodgement and potential ventricular capturing.
Figure 2. Vagal Stimulation Site For Endocardial Approach In The Human Heart.
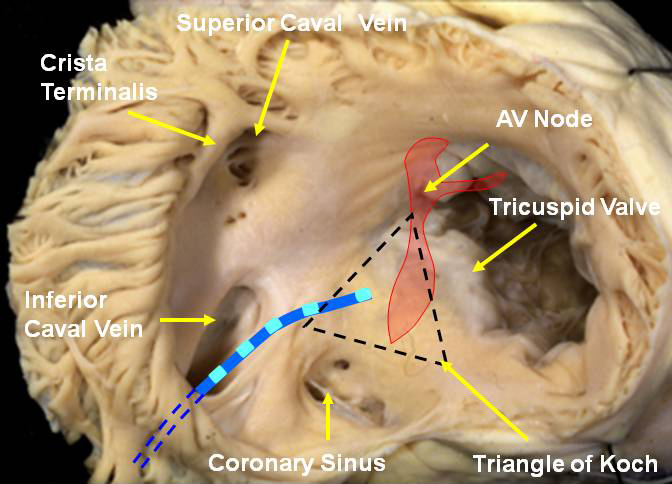
Click image for larger view.
A schematic diagram showing the site at the posterior right atrium at which optimal AV conduction delay could be achieved by electrical postganglionic vagal stimulation delivered with an endocardial catheter inserted through the inferior caval vein.(The diagram uses as a background a real anatomical image of endocardial view of human right atrium provided by Prof. R.H.Anderson.)
Selective AV Node Vagal Stimulation: Experimental Evidence
Although it has been known for a long time that cervical VNS can result in depression of AV node conduction, the application of selective AV node vagal stimulation to control ventricular rate during AF has been explored only during the last decade. Mazgalev et al.(43) demonstrated in vitro that when PGVS was applied directly onto the endocardial surface of the rabbit AV node, the depressive vagal effect could be maintained during simulated AF and resulted in controlled slowing of the ventricular rate.
A similar depressive effect on AV conduction can be achieved when electrical stimulation is applied epicardially to the AV node fat pad in dog hearts in situ. Wallick et al.(29) reported that in 11 anesthetized, open-chest dogs, selective AV node vagal stimulation through the epicardial approach produced slowing of the ventricular rate during AF that was associated with significant hemodynamic improvement. Zhang et al.(30) further demonstrated that by using a computer feedback controlled algorithm, different predetermined levels of ventricular rate slowing could be achieved and maintained by this approach. Thus an optimal ventricular rate during AF could be achieved with AV node vagal stimulation. It has been further demonstrated that ventricular rate slowing by selective AV node vagal stimulation was hemodynamically superior to currently used AV nodal ablation followed by regular right ventricular rate achieved with pacemaker.(31)
Long-term rate control by epicardial selective AV node vagal stimulation has been reported in chronic animals. Zhang et al.(32) studied 18 dogs in which chronic AF was induced using high-rate right atrial pacing. A pacing electrode was sutured to the epicardial AV node fad pad and AV node vagal stimulation was applied to the fat pad using implantable devices. Successful data were collected in 15 dogs. It was found that AV node vagal stimulation had a consistent effect on ventricular rate slowing (reducing ventricular rate by 40-50 bpm) during a 5-week observation period. In two of the dogs, the observations were extended to six months and the ventricular rate slowing effect persisted. It is of interest to note that the AV node vagal stimulation could be delivered continuously (impulses with duration 0.1 ms, 20 Hz) or as intermittent bursts synchronized with the QRS signal (a burst consists of 20 impulses, 1 ms duration and 6 ms interimpulse interval). The AV node vagal stimulation had almost instant ventricular rate slowing effect and the effect dissipated immediately after VNS was terminated (Figure 3). The vagally induced ventricular rate slowing was associated with improvement of hemodynamic responses. Importantly, AV node vagal stimulation therapy was well tolerated by conscious animals, causing no signs of distress or discomfort.
Figure 3. Surface ECG Recordings From A Chronic Dog Implanted With An AV Node Vagal Stimulation Device.
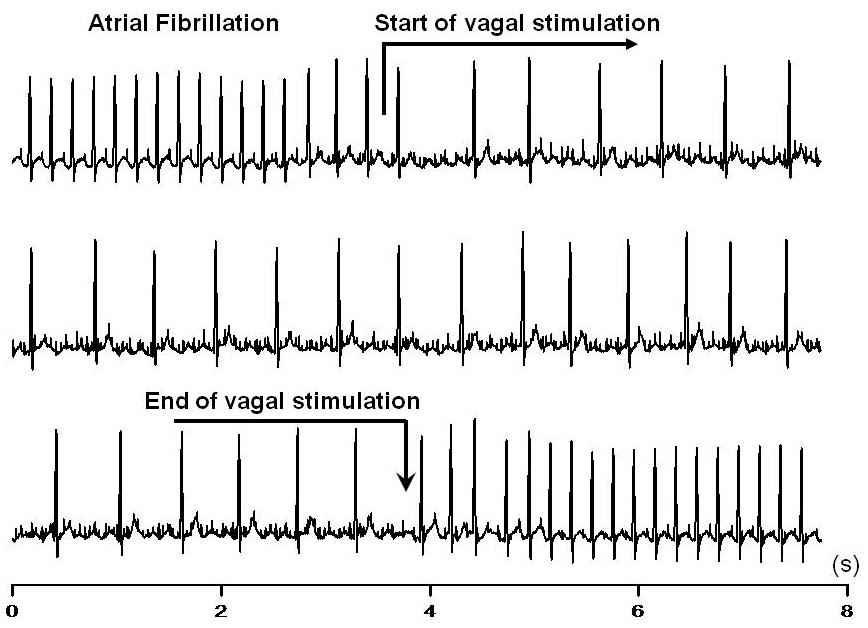
Click image for larger view.
The top trace shows at the beginning a rapid ventricular rate (≈240 bpm) during AF without vagal stimulation. The arrow indicates the start of vagal stimulation and the immediate resultant slowing of the ventricular rate. The middle trace shows the maintenance of slow ventricular rate (105 bpm) during continuous vagal stimulation. The bottom trace shows the prompt restoration of the initial (fast) ventricular rate after vagal stimulation was terminated (arrow).
In addition to the epicardial AV node vagal stimulation, selective AV node vagal stimulation has also been achieved through an endocardial approach using screw-in leads. By using a nonthoracotomy, transvenous technique, Mischke et al.(33) recently identified the projections of the right inferior ganglionated plexus (RIGP, the AV node fat pad) in nine dogs by using a specially designed probe and implanted an active-fixation lead endocardially. In five dogs weekly tests with intermittent high-frequency neurostimulation of the RIGP reproducibly yielded a negative dromotropic effect for six months resulting in an average reduction of ventricular rate during AF from 305 ± 7 bpm to 132 ± 28 bpm. In four dogs, AF was induced and maintained by rapid atrial pacing. Continuous VNS was applied and was shown effective in decreasing the ventricular rate during AF to a range of 100–140 bpm for one year in all four dogs. Two of the dogs were observed for two years and the rate slowing effect persisted. The VNS was well-tolerated during 1–2 year follow-up with a stimulation voltage <5 V. It was concluded that chronic vagal stimulation is safe, effective and well tolerated in the long-term control of ventricular rate in AF. The AV node selectivity and the opportunity to adjust the negative dromotropic effect within seconds may represent an advantage over pharmacological rate control.
Selective AV Node Vagal Stimulation: Clinical Data
The idea that selective stimulation of vagal nerves to the AV node might be of therapeutic interest has been explored clinically as well. In 1993 Keim et al.(58) reported the effect of subthreshold burst stimulation (SBS) of postganglionic vagal nerves to the AV node during clinical electrophysiological studies in 13 patients with a steerable mapping catheter. SBS resulted in transient intranodal conduction delay, which was dependent on the current strength. SBS-induced AV conduction delay was totally reversed by atropine, consistent with postganglionic vagal nerve stimulation and release of acetylcholine. The sites of selective vagal stimulation appeared discrete and localized within the triangle of Koch.
Schauerte et al.(48) reported vagal efferent nerve stimulation in 25 patients via a multipolar electrode catheter placed in the superior vena cava (SVC) or in the coronary sinus (CS). The catheter in the SVC was placed in such a position to avoid atrial capture. Vagal stimulation (20 Hz, 2 ms, 10-30V) in the SVC (n=14) induced negative chronotropic (slowing of sinus rate) and dromotropic (increased anterograde Wenckebach period) effects. In an AF patient, a significant ventricular rate slowing was observed during VNS. Vagal stimulation in the CS (n=11) was delivered with bursts (200 Hz, 50 ms duration, 10-30 V) in the atrial effective refractory period to prevent AF induction. A prolongation of the anterograde Wenckebach interval was observed with increasing voltage until third-degree AV block occurred in 8 of 11 patients. The authors concluded that autonomic modification of the AV nodal transmission may serve as an adjunctive tool for the diagnosis/treatment of supraventricular tachycardias and may be beneficial for ventricular rate slowing during tachycardic AF in patients with congestive heart failure.
In 2001, Quan et al.(54) studied the effect of endocardial parasympathetic nerve stimulation on the AV node conduction during AF (spontaneous or pacing-induced) in 18 patients. The endocardial catheter was positioned at the proximal coronary sinus or at the posteroseptal right atrium. It was found that stimulation at the posteroseptal right atrium in close proximity to the coronary sinus ostium (approximately 1 cm superior to the coronary sinus ostium) resulted in the greatest response, thus representing optimal site for stimulation of efferent parasympathetic nerve fibers to the human AV node (see Figure 2).
The feasibility and safety of endocardial stimulation of efferent AV nodal vagal fibers through placement of standard pacing lead to modulate AV conduction have been further explored in humans. Bianchi et al.(34) reported, in 12 patients with a history of AF and receiving implantable cardioverter-defibrillator, that an atrial lead implanted in the posteroseptal right atrium induced advanced AV block by temporary high-frequency stimulation (10 V, duration 0.2 ms, frequency 50 Hz ) applied through a diagnostic electrophysiology catheter. After implantation of a screw-in lead and connecting it to the implantable cardioverter-defibrillator, the effects of selective AV node vagal stimulation were tested by delivering 10-second trains of electrical impulses at different impulse durations (0.1– 0.5 ms) and increasing amplitude (up to a maximum of 8 V). The authors determined the minimum voltage needed to obtain complete AV block, defined as the occurrence of ventricular interbeat intervals greater than 1500 ms or as III degree AV block. In patients that were already in AF, or in which AF had been induced, the minimum voltage needed to obtain a 25% reduction in the mean ventricular rate was also determined.
It was found that AV block could be achieved in all patients, and ventricular rate modification in AF was achieved in nine patients. Furthermore, the effects of AV node vagal stimulation on AV conduction (i.e., modulation or complete AV block) remained reproducible after three months with no significant change in pacing thresholds. Only two lead dislodgments were reported in this first human study after three months, demonstrating that proper placement of the atrial lead can yield electrical characteristics suitable for permanent neural stimulation which could enable significant ventricular rate slowing by high frequency stimulation. The results were reproducible during follow-up, providing data for the development of device-based control of ventricular rate during AF.
In a separate study, Rossi et al.(35) reported in 20 patients with sick sinus syndrome (10 in sinus rate and 10 in AF) who were candidates for dual-chamber pacemaker implantation, that an "ideal" AV node vagal stimulation site at the posteroseptal right atrium could be identified by delivering high-frequency stimulation via a roving lead during atrial refractoriness. Delivery of AV node vagal stimulation at this site could achieve AV nodal conduction modulation (PR interval prolongation in the patients with sinus rate and ventricular rate reduction in the patients with AF). A pacing lead was subsequently screwed-in at the site and burst stimulation (pulse-rate 50 Hz, burst duration 180 ms) was delivered at different burst repetition-rates, pulse durations and amplitudes. In patients with sinus rate, PR interval prolongation was evoked at 90 and 120 bursts/minute with pulse durations ≤1 ms. Specifically, the mean voltages required to obtain PR interval prolongation and advanced AV block were 4.3±2.2V and 5.4±1.8V (at 90 bursts/minute and 1 ms impulse duration), respectively. Similarly, ventricular rate reduction was obtained in the AF patients, using neural stimulation with 90 bursts/minute, 0.5 ms pulse duration, and amplitude of 5.4±1.8V. Notably, no ventricular arrhythmias were induced during AV node vagal stimulation. It was concluded that endocardial burst AV node vagal stimulation successfully reduces ventricular rate during AF. Of interest, in sinus rate, employing a roving lead allows the optimization of lead positioning for AV node burst vagal stimulation.
There is a recent clinical case-report utilizing AV node vagal stimulation to suppress AV conduction during AF, which permitted resynchronization therapy with LV pacing. In this case Bianchi et al.(53) reported a patient with acute heart failure, chronic AF and uncontrollable ventricular rapid response, in severe hypotensive state secondary to cardiogenic shock. Ventricular rate control using standard therapeutic medications was considered inapplicable due to patient status. Thus, an atrial screw-in lead was implanted at the posteroseptal right atrium. The site was first identified with a diagnostic electrophysiology catheter by inducing functional AV block with high-frequency stimulation (10V, 0.2 ms, 50 Hz). The patient also underwent left ventricular pacemaker implantation. The delivery of AV node vagal stimulation fully inhibited AV conduction and permitted an uninterrupted LV pacing. The combined pacing strategy resulted in hemodynamic improvements and allowed subsequent β-blocker (carvedilol) titration. After four days, the ventricular rate could be controlled by carvedilol and the atrial lead was removed. The patient recovered satisfactorily. The authors conclude that this novel strategy may allow controlling the rapid AV response in patients undergoing pacemaker implantation.
Selective ganglionic AV node vagal stimulation has also been reported clinically to control ventricular rate in post-operative AF patients. Rossi et al.(59) studied 32 consecutive patients who underwent bypass surgery. A temporary heart wire was implanted in the epicardial AV node fat pad. Electrical stimulation of this fat pat evoked a functional AV block in 29 patients (91%). During post-operative AF, AV node vagal stimulation was delivered through the heart wire to decrease ventricular rate on-demand. Fourteen patients (44%) developed post-operative AF. In these patients, AV node vagal stimulation achieved a 25% reduction of ventricular rate and complete AV block with 6.0 ± 1.9 V and 7.5 ± 1.8 V (duration 0.2 ms, frequency 50 Hz), respectively. It was concluded that epicardial AV node vagal stimulation represents an effective and promising technique to decrease ventricular rate during post-operative AF.
Remaining Challenges
Despite the substantial progress being made in both experimental and clinical studies utilizing selective AV node vagal stimulation to control ventricular rate during AF, and the determination that stimulation parameters (voltage, impulse duration and stimulation frequency) required to achieve ventricular rate slowing are within the capacity of conventional pacemakers,(52) much more remains to be done before this technique can become a routine clinical practice.
First, the long-term effects of AV node vagal stimulation (either endocardial or epicardial approach) on ventricular rate control in patients remain to be elucidated. Although data accumulated in experimental studies have shown the feasibility of long-term chronic AV node vagal stimulation, the long-term clinical data in patients are still missing and remain to be formally established
Second, further development of implantable neurostimulation technology, including devices and leads, is needed. Currently, devices and leads used in different reports were "borrowed" from cardiac pacing inventory (such as implantable cardioverter-defibrillators), not specifically designed for neurostimulation purposes. Although Soos et al.(52) found that cardiac neurostimulation follows the chronaxie/rheobase relationship, there are differences in the desired stimulation parameters for neurostimulation. The chronaxie (0.14-0.18 ms) is about half of that for myocardial stimulation but the rheobase is roughly doubled. More importantly, the biological effect of vagal stimulation (e.g., acetylcholine release) is not directly coupled to the parameters of single electrical stimulus but to the cumulative effect of a series of high-frequency stimuli. As a result, the maximal ventricular rate slowing is usually achieved at stimulation frequency of 30-50 Hz, which corresponds to 1800-3000 impulses/min or at least 10 times faster than regular myocardial pacing. As a consequence a pacemaker-type battery would be depleted in roughly six months. Thus, a substantial change in battery technology is required to prolong the device life for neurostimulation, which certainly could happen.(52)
In addition, it would be desirable that the neurostimulator deliver automatically adjusted feedback controlled stimulation parameters to achieve ventricular rate slowing dependent on the patients's needs. Such a device is technically possible based on sensor-feedback technologyl.(30)(51)
Currently, conventional pacemaker leads have been used for neurostimulation. However, selective AV node neurostimulation may require exciting a relative large area compared with myocardial pacing, since neurostimulation should reach as many neurons and nerve fibers as possible in the ganglionated plexus. Thus, specifically designed electrodes (both for endocardial or epicardial stimulation) may facilitate electrode implantation and offer optimized long-term effects. Early data indicate that stimulation electrode actively fixed inside the neural plexus may substantially reduce energy needed for nerve excitation, as compared to a transvenous catheter just placed on the endocardial surface.(48)(52)
On the other hand, lead dislodgement and potential inadvertent high frequency ventricular pacing remain serious concerns in cases of endocardial lead placement.(34) Advances in lead design and fixation technology may resolve these problems.
Finally, because of the lack of long-term clinical data in patients, side effects associated with neurostimulation remain to be established. Although animal studies have shown no obvious side effects associated with AV node vagal stimulation,(30)(33) given the complexity of intrinsic cardiac autonomic system and possible interactions between different ganglionic plexi,(60)(61) the clinical tolerability of this novel approach needs future investigation.
Conclusion
Although more clinical studies are needed to establish the role of selective AV node vagal stimulation as a vital therapy for ventricular rate control during AF, initial clinical studies, along with the rich body of experimental data accumulated during the last decade, suggest that AV node vagal stimulation could be a novel therapy for modulation of the AV node transmission in AF. Selective AV node vagal stimulation offers a rapid, almost instant effect, with fast and complete reversibility. It also provides programmability and desired flexibility of rate control. Thus, this novel approach has obvious advantages, compared with other treatments such as medications, and may offer transient or longer-term control of the ventricular rate in certain population of patients with AF.