Course Authors
David Avigan, M.D.
Release Date: 12/06/2007
Upon completion of this Cyberounds®, you should be able to:
Identify the unique biological characteristics of AML in the elderly and their impact on response to therapy
Discuss therapeutic trials in elderly patients with AML which examine the role of aggressive and low intensity chemotherapy
Define the role of autologous and allogeneic hematopoietic transplantation in elderly patients with AML
Discuss the role of novel agents as therapy for elderly patients with AML.
Dr. Avigan will discuss investigational trials for AML.
Acute myeloid leukemia (AML) is a hematological malignancy with considerable biological heterogeneity. The American Society of Hematology image bank contains 95 sets of image showing the wide variety of morphologic features. A series of prognostic factors have been identified that predict for sensitivity to chemotherapy, risk of treatment-associated morbidity and long-term outcomes. These include measures of disease bulk (white blood cell count and lactate dehydrogenase levels), assessment of patient comorbidities (serum bilirubin and creatinine levels), and the intrinsic biology of the malignant clone (history of an antecedent hematological condition or treatment-induced leukemia, cytogenetic abnormalities, and sensitivity to induction chemotherapy).(1)(2)(3)(4)(5)(6)(7) This has been reviewed in the ASH Education Book of 2006.
Epidemiology
Acute myeloid leukemia is primarily a disease of the elderly with a median age of 65.(8) See graph of SEER data outlining the incidence. In 2000-2003, USA incidence was 1.8/100K for age <65 and 17/100k for 65 and over.(9) AML in the elderly represents a distinct biological and clinical entity which poses a significant challenge to the clinician. Advanced age is considered a negative prognostic indicator resulting from both the decreased capacity of patients to tolerate chemotherapy and its correlation with more aggressive underlying disease biology.
Elderly patients demonstrate increased treatment-associated morbidity and mortality because of more limited organ reserve, susceptibility to regimen-related toxicity, and decreased capacity to withstand infectious complications that manifest during the prolonged period of treatment-induced neutropenia. AML in the elderly more commonly evolves from an underlying myelodysplastic syndrome and is often associated with complex cytogenetic abnormalities. As a result, AML in the elderly is associated with decreased sensitivity to standard induction chemotherapy, resulting in inferior rates of complete response with poor durability. Complete remissions are observed in <60% of whom >85% demonstrate evidence of disease progression within 3 years.(4)(10)(11)
Outcomes reported from trials performed at tertiary care centers may not fully represent what is observed in community practice. In one review of leukemia studies performed by the SWOG,(12) patients >65 represented only 27% of study population while they are thought to represent 50-60% of the patients with AML. Reported outcomes are impacted by the intrinsic selection bias in which elderly patients are judged eligible for intensive chemotherapy.(13)(14)(15)
In a review of 2657 elderly patients with AML collected by the Surveillance, Epidemiology and End Results (SEER), median survival was only 2 months with a 2-year survival of 6%, significantly worse than that reported by cooperative group trials.(16) Reviews of trends in survival also fail to show any improvement in older patients. Standard chemotherapy for younger patients with AML has consisted of infusional cytarabine in combination with anthracycline therapy. Use of less intensive chemotherapy has not been examined with palliative intent but no standard of care therapy has emerged that results in significant rates of sustained remissions in elderly patients unable to tolerate aggressive chemotherapy.
Characteristics and Prognosticators
Several features of AML in the elderly suggest that it characteristically evolves from a primitive progenitor with phenotypic characteristics similar to hematopoietic stem cells.

Figure 1. Bone Marrow Biopsy Is Markedly Hypercellular in This Elderly Patient (H & E).
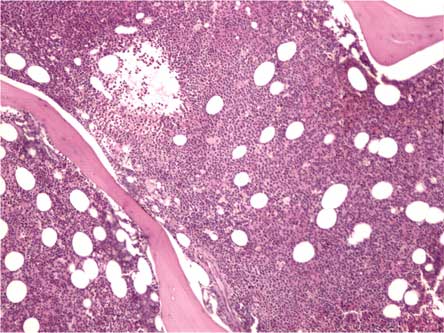
Maslak, P. ASH Image Bank 2004;2004:101230.
Copyright © 2004 American Society of Hematology. Copyright restrictions may apply.
AML commonly evolves from myelodysplastic syndrome (MDS) consistent with the concept of a clonal disorder originating from a stem cell abnormality.
Figure 2. Dysplastic Erythroid and Myeloid Elements Are Seen Along with the Blasts.
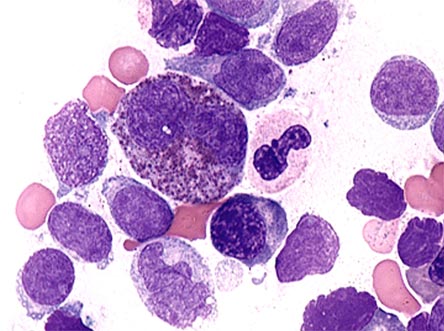
Maslak, P. ASH Image Bank 2004;2004:101177.
Copyright ©2004 American Society of Hematology. Copyright restrictions may apply.
Stem cells typically demonstrate a low proliferative phenotype rendering them more resistant to toxin-mediated injury and chemotherapy-induced DNA damage. A variety of biological mechanisms further protect primitive malignant cells including the enhanced efflux of chemotherapeutic agents via the multi-drug resistant (MDR) pathway.(17)(18) Expression of the MDR1 phenotype is associated with a complex cytogenetic pattern. In a study of 211 patients with AML, myeloid leukemia cells derived from elderly patients are characterized by the increased presence of the MDR phenotype.(19) In another study, the MDR phenotype was present in approximately 30% of younger patients and 57-62% of older patients.(20) Other mediators of biologic resistance such as expression of BCL2, reduced susceptibility to apoptosis, mutations in the p53 gene and expression of a stem cell phenotype (CD34) by the leukemic clone may all contribute to increased biological resistance to therapy.(21)(22)
Cytogenetics has been identified as a highly significant prognostic factor determining outcome in patients with AML. t(8;21)(q22;q22), inv(16) (p13q22) or t(15;17) (q22;q11-12) are considered favorable patterns while -5/del(5q), -7/del(7q),inv(3)/t3;3) or complex aberrations predict for poor outcomes.(2)(4)(17)(23)
Figure 3. Spectral Karyotype Analysis of a Metaphases From Bone Marrow Specimen From a Patient with Acute Myeloid Leukemia Showing Complex Chromosome Abnormalities.
Left panel, spectral image; Right panel, classified colors.
Courtesy of Vundavalli Murty, Ph.D.
Patients without identifiable chromosomal aberrations are considered to in the intermediate risk category. For example, a Medical Research Council (MRC) study analyzing outcomes in 1612 patients under age 55 undergoing intensive treatment demonstrated that 5-year risk of relapse was 35%, 51% and 76% and survival was 65%, 41% and 14% for patients falling into the good, intermediate and poor risk cytogenetics groups, respectively.(17)
Figure 4. MRC AML 10 Study.
Grimwade D, et al. Blood. 1998;92:2322-2333.
Similar differences were observed in other large cohorts including a Cancer and Leukemia Group B (CALGB) study of 1213 patients.(2)
Significant efforts have focused on further refining the biological characterization of the disease to better define outcomes and guide therapeutic decisions, particularly in patients with normal cytogenetics. FLT-3 protein is expressed in early hematopoietic progenitors which may demonstrate internal tandem duplications (ITD) in 20-30% of patients with AML.(24) This results in constitutive activation of FLT-3 mediated signaling of pathways that impact cell proliferation. Of note, in a study of 854 patients with AML, the presence of the internal duplications of the Flt3 gene was seen in all cytogenetic categories and was an independent negative prognostic marker with respect to rates of complete remission (CR), treatment-associated mortality, risk of relapse and overall survival.(25)
Figure 5#. Prognostic Significance of FLT3 Internal Tandem Duplication.
Kottaridis PD, et al. Blood. 2001;98:1752-1759.
Presence of internal tandem duplications of the FLt3 oncogene also results in lower relapse-free survival in older patients. BAALC expression is also predictive of poor outcomes and in the context of FLT-3 mutations defines a particularly poor prognosis group. In contrast, mutations of the C/EBPα or NPM genes occur in 15% and 35% to 50% of patients with AML, respectively, and are associated with improved outcomes.(26)(27)
Cytogenetic categories retain their prognostic significance in the elderly population in whom unfavorable cytogenetic patterns are more common.(4)(23)(28) As a follow up to the MRC AML 10 study, which identified cyogenetics as highly predictive of outcome in younger patients with AML, investigators in the UK studied the impact of karyotype on outcome for 1065 cases of AML in older adults (median age 66) in the MRC AML 11 study.(23) Cytogenetics remained an important predictor of outcome in older patients with AML. Favorable cytogenetic patterns were identified in only 7% of cases, significantly fewer than that observed with younger patients in the MRC 10 study, and were frequently associated with additional abnormalities. In contrast, there was an increase in patients with normal and complex karyotype in older patients.
Advanced age retained its negative prognostic significance across all of the cytogenetic categories. A majority of patients were classified as being in the intermediate risk cytogenetics group while approximately 20% of patients exhibited poor risk cytogenetics which frequently manifested as complex karyotypes. Patients with good risk cytogenetics demonstrated improved rates of CR but 5-year survival was only 34%, statistically inferior to that observed with younger patients. Of note, outcomes in patients with acute promyelocytic leukemia (APL) were worse in older patients as a consequence of a high rate of early death in the setting of brief course of all trans-retinoic acid (ATRA).
In contrast, other studies have demonstrated excellent results in elderly patients treated with more extended ATRA.(29) CR rate was 60% for the intermediate group with a higher associated incidence of resistant disease. Long-term survival was 15% in this group. In the poor risk cytogenetic category, only 32% of patients achieved CR, 51% demonstrated primary resistant disease and overall survival was only 4% at 5 years. In contrast to younger patients, complex cytogenetics demonstrated worse outcomes (overall survival of 2%) than individual abnormalities associated with poor risk.
In a German study, 1225 patients with de novo AML were studied to assess the effect of cytogenetics on outcome within different age groups.(7) Three hundred thirty-three patients were between 60-69 years old and 204 were older than 70. The incidence of t(15;17), t(8;21), and inv(16) each decreased across the age groups, while complex karyotypes increased. Rates of complete remission declined progressively with advancing age. Cytogenetics remained prognostically significant for predicting survival within each of the elderly groups. For patients with good prognostic cytogenetics, survival was significantly worse for patients older as compared to those younger than 60.
Response to Conventional Treatment
The role of standard induction chemotherapy in the treatment of elderly patients with AML remains controversial because of the inferior rates of complete response that are observed and poor durability of response.(30) Lowering the intensity of chemotherapy has improved treatment-associated mortality, but at the expense of therapeutic efficacy, resulting in a lack of improvement in response. Only a few randomized studies have been conducted in this population to assess relative outcomes following aggressive chemotherapy as compared to supportive care or low dose therapy.
In a study published in 1989 of elderly patients with AML who demonstrated adequate organ function and performance status, aggressive chemotherapy was associated with improved median survival (21 weeks), as compared to those receiving supportive care alone (11 weeks).(31) Both groups were hospitalized for a similar number of days. Of note, survival was poor in both arms of the study. In another study, patients over the age of 65 were randomized to receive low dose cytarabine for 21 days as compared to rubidazone for 3 days in conjunction with cytarabine at 100 mg/m2 for 7 days.(32) Although intensive therapy was associated with a higher incidence of CR, overall survival was not improved as a result of higher rates of treatment-related mortality in the aggressive therapy arm. Long-term survival rates remained poor. As such, no clear indication for the use of aggressive chemotherapy is provided by the limited randomized studies that have been performed.
A larger series of retrospective studies has addressed the question as to role of aggressive chemotherapy in the treatment of the elderly.(30)(33)(34)(35)(36)(37) Several studies have suggested that supportive care alone or low intensity therapies are preferable in older patients, particularly those older than age 75, while others have found benefit in selected patients identified by prognostic criteria. Factors such as presence of abnormal cytogenetics and presence of MDR gene predict for response to therapy.(6)(17)(38) Presence of complex cytogenetics, antecedent hematological disease, and elevated WBC count have also been shown to predict outcome in elderly patients. In a summary review of studies examining the impact of regimens consisting of anthracycline and cytarabine of nearly 2000 elderly patients, complete response rates ranged from 40-60%, induction mortality was 15-20% and long-term survival was 8-12%.(33)
An Italian study reported on outcomes of 1005 AML patients older than 60 (median age 69) treated between 1992 and 1998.(39) Six hundred twenty-one patients received intensive therapy predominantly consisting of anthracycline and cytarabine with or without the addition of etoposide. The remaining 384 patients were managed conservatively including low dose cytarabine, hydroxyurea, 5-azacytidine or supportive care only. The supportive care group demonstrated poor risk features with respect to mean age, performance status, cardiac comorbidity and previous MDS. Overall 1-year survival for the whole group was 28%. Median survival was 7 and 5 months and 1-year survival was 31% and 21% for the intensive and supportive care groups, respectively (p<0.001). In patients over age 70, no survival difference was seen between the two groups, despite imbalance of risk factors favoring outcome in the more aggressively treated group. No survival differences were observed between intensive treatment regimens or within the supportive care options. Those patients with the best risk factors showed better mean survival but no advantage with aggressive therapy. In contrast, patients with an elevated WBC (>10), but otherwise good risk factors, benefited from aggressive therapy. Duration of hospitalization was twice as long for the aggressively treated group.
Given the poor outcomes with aggressive chemotherapy for the entire cohort of elderly patients with AML, investigators have examined whether a particular subgroup of patients may benefit from induction chemotherapy. Kantarjian et al. reported on outcomes of 998 patients age 65 or older with AML (80%) or high risk MDS (20%) who were treated with intensive chemotherapy.(40) Median age was 71. Fifty-four percent of patients demonstrated unfavorable cytogenetics. Forty-five percent of patients achieved CR with 29% of patients dying during induction. The median survival was 5.4 months with 1- and 2-year survival of 30% and 16%, respectively.
In multivariate analysis, older age, poor performance status, complex cytogenetics, treatment outside laminar air flow room, elevated creatinine and antecedent hematological disorder ≥12 months were identified as independent poor prognostic factors. By these criteria, patients could be subdivided into cohorts for which early mortality was ≤10% for patients without negative factors (20% of patients), 1-2 negative factors experienced a mortality rate of 27%, (56% of patients), and those with ≥3 factors had a mortality ≥60% (24% of patients). Similarly, 1-year overall survival ranged from >60%, 33%, and <10% for patients with no adverse factors, 1-2 factors and ≥3 factors, respectively.
Of note, a retrospective study from the GIIMEMA (Italian Multiple Myeloma Network) group failed to show significant improvement in outcome in patients treated with aggressive chemotherapy, despite the demonstration of improved prognostic markers relating to performance status, median age and antecedent hematologic disease in this group.(39) The intensively treated group had only a 2-month improvement in survival and a 2-fold increase in days of hospitalization. Among patients achieving CR, one study demonstrated an improved disease-free survival (DFS) but not overall survival (OS) with low dose cytarabine, as compared to observation. In a CALGB study comparing 3 levels of intensity for cytarabine-based consolidation, no differences were seen for patients over age 60, with an overall DFS of only 14% for the cohort.(41) Consolidation therapy has not been shown to improve outcomes in older patients.(42) In summary, while a subset of elderly patients may benefit from intensive therapy, overall outcomes remain poor and novel treatment strategies are needed.
Hematopoietic Growth Factors
The use of hematopoietic growth factors has been explored to improve toxicity associated with aggressive chemotherapy or, alternatively, in an effort to enhance responses by stimulating leukemia blasts to go into cell cycle. In a randomized study of 124 patients older than 55, standard induction therapy was administered alone in conjunction with GM-CSF, which was initiated after documentation of bone marrow aplasia. The GM-CSF arm was associated with decreased period of neutropenia, decreased infectious complications and improved survival.(43) Multiple studies have confirmed that growth factor administered after chemotherapy shortens chemotherapy-induced neutropenia but have not demonstrated an impact on outcome or infectious complications.(44)
In a study of 240 patients with AML, age 55-75, use of GM-CSF with induction chemotherapy did not improve the CR rate but was associated with improved 2-year DFS.(45) Lowenberg et al. demonstrated that G-CSF administered prior to induction and consolidation chemotherapy was associated with improved DFS and decreased relapse rate in patients with AML less than age 60 who achieved a complete response (Figure 6).(46) No improvement was noted in poor risk disease and overall survival was unchanged. In a subsequent trial, 722 patients with median age of 68 were randomized to receive no G-CSF, G-CSF in conjunction with chemotherapy, following chemotherapy, or both during and following chemotherapy.(47) A higher CR rate was observed in patients treated during chemotherapy but no overall advantage was seen in overall or disease-free survival.
Figure 6. Disease-Free Survival in AML with or without G-CSF Priming.
Löwenberg B, et al. N Engl J Med. 2003;349:743-752.
Autologous Transplant
High dose chemotherapy with stem cell rescue has been shown to be an effective means to decrease risk of relapse through intensification of chemotherapy dose. Several randomized studies have compared outcomes to that observed following standard chemotherapy.(48)(49) The autologous transplant arm has consistently demonstrated better disease control but at the expense of increased treatment-related mortality with differing conclusions regarding the overall effect on outcome. Several studies have demonstrated the feasibility of autologous transplant in patients over the age of 60. However, in a review of data from the European bone marrow transplant registry, patients over age 50 (n=11) experienced an inferior leukemia-free survival and overall survival as compared to younger patients (n=786). Although risk of relapse was not different between the 2 groups, transplant-related mortality was higher in older patients, predominantly from infectious complications.(50) In a second study, results following autologous transplantation for 193 patients over the age of 60 were presented.(51) A majority of patients (147) were in CR1. LFS and OS at 3 years was 36% and 47%, respectively. Of note, the risk of relapse was decreased for patients receiving bone marrow, as compared to peripheral blood stem cells, and outcomes were improved in patients transplanted more recently.
The difficulties in advancing elderly patients towards autologous transplantation and the inherent selection bias of the results were demonstrated in a study by the Catalan Leukemia Group.(52) Of 135 patients assigned to the aggressive chemotherapy, only 16 patients ultimately received a transplant as a result of inability to collect stem cells, early relapse or other medical issues. Of note, the leukemia-free survival (LFS) was superior in patients proceeding to transplant (39% vs. 22%), signifying in large part the effect of selection bias.
In a study of the EORTC-GIMEMA group, 278 patients with AML age 61-70 were treated on a protocol calling for autologous transplantation for patients in remission following induction and consolidation therapy.(53) Of these patients, 132 patients were in remission following consolidation but a majority of patients did not proceed with stem cell collections. Thirty-eight of fifty-four (38/54) patients who underwent collection obtained adequate yields and ultimately 35 patients underwent transplant. Disease-free survival at 3 years was 28%, which was not superior to those patients who had received consolidation therapy alone. The difficulty in completing autologous transplant for a majority of patients was also highlighted in a study of 155 patients with AML over age 60 being considered for aggressive chemotherapy and transplant in which only 13% underwent transplantation.(54) At this time, the impact of autologous transplant on outcome in this age group remains uncertain.
Allogeneic Transplantation
Allogeneic transplantation demonstrates unique efficacy in AML through the potential eradication of disease via the graft versus disease effect. Historically, allogeneic transplant was previously limited to younger patients because of the significant treatment-associated morbidity and mortality with increased risk demonstrated by older patients. Older patients are more susceptible to regimen-related toxicity and demonstrate an increased incidence of graft versus host disease (GVHD).(55)
In a report from the Seattle group, 52 patients with AML and MDS greater than age 60 underwent myeloablative conditioning followed by allogeneic transplantation.(56) Non-relapse mortality was 27% and 43% at 100 days and 3 years. At a median of 4.6 years of follow up, 18 patients remained disease-free. Of note, no patients with advanced disease at time of transplant survived. Ringden et al. reported that patients with early stage leukemia demonstrate a similar non-relapse mortality between age 45-49 and greater than age 50 following a myeloablative conditioning regimen.(57) However, older patients with advanced disease experienced a markedly increased rate of mortality. In another report, 215 patients with hematological malignancies who were over the age of 50 underwent allogeneic transplantation following ablative conditioning. Ten-year survival and 1-year treatment-related mortality were estimated at 56% and 30% respectively.(58) However, outcomes were significantly worse for those patients with advanced disease. Investigators have explored approaches to reduce treatment-associated toxicity of ablative regimens by modifying the intensity of regimen. In one protocol, patients with myelodysplastic syndrome greater than age 60 demonstrated good outcomes by targeting busulfan doses to a steady state plasma concentration of 900 ng/mL.(59)
A major focus of investigation to reduce transplant-related morbidity and mortality and to increase transplant accessibility for older patients is the use of reduced intensity regimens for transplant conditioning (RIC). Data from highly selected cohorts of older patients have yielded promising results with limited follow up.(55)(60)(61)(62)(63)(64) The Seattle Consortium reported on the outcomes of 122 patients with AML treated with low dose TBI and fludarabine.(65) Patients were generally considered ineligible for a standard ablative transplant because of age and/or medical comorbidities. Engraftment was achieved in 95% of patients. The cumulative incidence of moderate to severe aGVHD (acute graft versus host disease) was 35% and 42% following transplantation from a related and unrelated donor, respectively. Treatment-related mortality was 10% and 22% following related and unrelated transplants, respectively. The overall 2-year disease-free and overall survival was 44% and 48%, respectively. Improved outcomes were observed for patients transplanted in CR1. Of note, outcomes after unrelated transplants were not inferior possibly because improved graft versus leukemia effects counterbalanced increased non-relapse mortality. In another study, 37% patients with AML or MDS remained alive at a median of 3.7 years of follow up, including a high percentage of patients with secondary AML who were in remission at the time of transplant.(66)
In a German multicenter study, the probability of DFS following RIC transplant was inversely correlated with disease burden.(67) In a report of 112 patients with AML or MDS transplanted with RIC at M.D. Anderson (median age 55), the 2-year survival was 66%, 40% and 23% for patients treated in CR, with active disease but without circulating blasts, and for those with circulating leukemic blasts, respectively.(68)Of note, non-relapse mortality also correlated with status of disease at transplant.
Investigators have attempted to improve outcomes following RIC using T cell depletion to minimize toxicity secondary to GVHD. In two studies, patients with AML or high risk MDS were treated with alemtuzumab in addition to RIC.(69)(70) GVHD was limited but disease relapse was noted as the most common cause of treatment failure. Outcomes were best in patients with disease who were at lower risk for relapse.
Another approach to improve outcomes in patients with more advanced disease is combining RIC with more intensive pre-transplant cytoreduction and post-transplant prophylactic donor lymphocyte infusion. In a report of 75 patients with AML or MDS, this strategy resulted in a 2-year DFS of 40% without worse outcomes noted in patients with poor prognostic factors at time of transplant.(71) In a series of retrospective studies, investigators have compared outcomes following RIC vs. ablative conditioning.(72) These studies have demonstrated decreased treatment-related mortality with RIC and a corresponding increase in risk of relapse resulting in similar long-term outcomes. These studies conclude that RIC was a feasible alternative to ablative therapy, though the appropriate application toward elderly patients needed to be further clarified.
The potential importance of the graft versus disease effect in improving outcome for elderly patients with AML was highlighted in a recent report comparing outcomes in patients over age 50 undergoing RIC allogeneic transplantation (n=316) to those undergoing high dose chemotherapy with autologous stem cell rescue (n=1369).(73) After correcting for disease-related factors by multivariate analysis, patients undergoing RIC demonstrated improved LFS and OS. No advantage was seen in patients transplanted in first complete remission (CR1) because the lower relapse rate-associated allogeneic transplantation did not compensate for the higher treatment-related mortality. However, improved outcomes were observed in patients with more advanced disease.
Despite encouraging results reported in some elderly patients undergoing allogeneic transplantation, its general applicability to this patient population remains uncertain. Estey et al. assessed the feasibility of transplanting patients over the age of 50 by tracking outcomes in all potentially eligible patients at M.D. Anderson beginning at time of diagnosis.(74) Of 259 patients treated with AML or high risk MDS, 99 patients entered CR. Only 53 patients were evaluated by the transplant service because of issues related to patient illness, donor availability or preference. Donors were identified for 26 patients and transplant was ultimately performed in only 14 patients. Of note, in a case-controlled comparison with patients treated with chemotherapy, those patients undergoing transplantation did demonstrate improved survival.
Novel Agents
In an attempt to improve on the poor outcomes demonstrated with conventional chemotherapy, novel agents have been explored as therapy for patients with elderly AML. Gemtuzumab ozogamicin is an antibody directed against the myeloid CD33 antigen bound to a chemical toxin colicomicin. In a series of phase II studies, 142 patients with relapsed AML underwent therapy, including 80 patients over age 60. In this cohort, 15% of patients achieved a CR and an additional 11% demonstrated eradication of leukemia cells with incomplete recovery of normal hematopoietic elements. Elderly patients demonstrated a shorter relapse-free survival as compared to younger patients. Toxicity was predominantly related to infusional reactions and myelosuppression. Hepatotoxicity has emerged as an important concern particularly in patients who are subsequently treated with stem cell transplantation. Gemtuzumab ozogamicin is currently being examined as a part of combination chemotherapy regimens.(75)
Given the association of the MDR phenotype with poor outcome and its relative prevalence in older patients with AML, investigators have examined the efficacy of MDR inhibitors in conjunction with chemotherapy. Early studies with cyclosporine A (CSA) demonstrated conflicting results. A phase II study of CSA, daunorubicin and cytarabine demonstrated a CR rate of 62% in poor risk patients.(76) In a phase III study conducted by SWOG, use of CSA was associated with improved disease-free and overall survival.(18) Other studies failed to confirm these findings. Another inhibitor, PSC-833, was associated with increased treatment-related mortality and did not result in improved outcomes.(77)
Hypermethylation abnormalities have been noted in myeloid leukemia cells and may be associated with the inactivation of tumor suppressor genes. Inhibitors of DNA methyltransferases such as azacytidine and decitabine (5-aza-2'-deoxycitidine) have been explored as therapy for AML. Several studies(91)(92)(93)(94)(95)(96) have demonstrated the efficacy of azacytidine and decitabine in relapsed or refractory leukemia and myelodysplastic syndromes.(78)(79)
Tumor angiogenesis represents another potential novel target for AML therapy. Increased microvessel density has been noted in bone marrow biopsies of AML. Vascular endothelial growth factor (VEGF) stimulates growth of leukemic cells, and increased serum levels are associated with poor outcomes. In a phase II trial, the efficacy of a small molecule that inhibits phosphorylation of VEGF receptors, SU5416, was examined.(80) Forty-three (43) patients with refractory disease or elderly patients not appropriate for standard therapies were enrolled. Although the clinical effects were modest, responses were linked with higher levels of VEGF expression by leukemia blasts and were associated with decreased microvessel formation in the bone marrow.
BCL2 is an inhibitor of apoptosis and high levels of expression in AML is associated with poor response to therapy. A phase I trial of a BCL2 antisense oligonucleotide demonstrated evidence of response in patients with refractory disease.(81) A subsequent trial demonstrated feasibility of combining this agent with chemotherapy. A randomized study is being performed to assess its role in augmenting response to induction chemotherapy.
Alternative cytotoxic therapies are also being examined as therapy for elderly patients with AML. Clofarabine (note: PDF) is phosphorylated to an active metabolite, clofarabine triphosphate, which inhibits DNA polymerases and ribonucleotide reductase. Clofarabine alone or in combination with cytarabine has shown activity in patients with AML.(82)(83)(84) In a phase II study of patients with recurrent or refractory acute leukemia, 13/31 patients with AML achieved a CR. Responses were more commonly seen in patients with a longer disease-free interval prior to therapy. A phase I-II study examined the toxicity of efficacy of a 5-day course of clofarabine in combination with cytarabine 1 gm/m2 in patients with relapsed or refractory acute leukemia, including 25 patients with AML. Twenty-two and 16% of patients achieved CR and CRp (CR with incomplete platelet recovery), respectively. An increase in ara-CTP was noted in the leukemic blasts:(83) Similarly, the novel agent VNP40101M has shown efficacy in elderly patients with AML.(85)
Another novel treatment approach involves the use of histone deacetylase inhibitors that induce gene expression and may promote the differentiation and growth arrest of malignant cells. In one example, MS-275 has been shown to increase expression of genes that inhibit proliferation (p21) with associated in vitro activity against leukemia cell lines.(86) In a recently published phase I study of 38 patients, treatment was associated with acetylation of proteins with increased expression of p21 but no clinical responses were observed.(86)
Farnesyl transferase inhibitors (FTIs) target ras-mediated signaling and a variety of other pathways that are essential for mitosis, cell survival, angiogenesis and cell adhesion. In one study, 158 elderly patients with median age of 74 years old were treated with tipifarnib, an oral FTI.(87) The majority of patients had an antecedent MDS. Fourteen percent (14%) of patients experienced a CR with a median duration of 7.3 months and median survival of 18 months. Seven percent (7%) of patients experienced early mortality that was unrelated to progressive disease. CRs were not seen in patients in whom inhibition of FTase was undetectable. While significant responses were seen in only a minority of patients, the ability to effectively target AML in a relatively resistant population was encouraging.
Patients with AML with mutations in the genes encoding for FLT3 demonstrate increased biological resistance to standard therapies. Inhibitors of FLT3 tyrosine kinase, including PKC-412 and lestaurtinib, are being explored as therapy for AML alone or in conjunction with chemotherapy.(88)(89) In a recent study, the toxicity and efficacy of tandutinib, an oral inhibitor of type III receptor kinases including FLT3, was examined.(90) Forty (40) patients with a mean age of 70.5 were treated. Evidence of inhibition of FLT3 phosphorylation was observed. Two of five patients treated at the maximum tolerated dose demonstrated reduction in circulating and bone marrow blasts. The presence of biological effects of FLT3 inhibition suggests that further examination of these agents alone or in conjunction with other therapy may be warranted.
The most significant prognostic factor for patients with AML is the pattern of chromosomal changes observed in the leukemic clone. Abnormalities of the core binding factor genes are found in patients with inv (16) and t(8;21) and are associated with improved response to chemotherapy and survival. t(15;17) is found in acute promyelocytic leukemia which demonstrates high rates of durable response to combination therapy with all trans-retinoic acid (ATRA) and chemotherapy. Patients with normal cytogenetic findings are considered to be in the intermediate prognostic group. Complex cytogenetic abnormalities and deletions of chromosome 5 or 7 are associated with poor outcomes and may be associated with antecedent myelodysplastic syndrome.
Multiple prognostic factors contribute to the poor outcomes observed with older patients. AML commonly exhibits a more primitive phenotype that is associated with greater biological resistance to therapy. Consistent with this picture is the increased frequency of the multi-drug resistance phenotype, complex cytogenetic aberrations and antecedent myelodysplastic syndrome. Co-morbid conditions frequently limit the capacity of these patients to tolerate aggressive chemotherapy. FLT3 mutations are found in a significant proportion of patients with AML and are associated with worse prognosis in the setting of otherwise normal cytogenetics.
Poor outcomes following standard chemotherapy have been observed in elderly patients with AML. The role of consolidation therapy has not been established and the benefit of high dose cytarabine has been demonstrated in patients under age 60. Few randomized studies have compared aggressive chemotherapy with supportive care and results are mixed. Patients treated with aggressive chemotherapy demonstrate modest or no improvement in survival as compared to those receiving supportive care or reduced intensity treatment. Some studies have defined subgroups that may show better responses to aggressive chemotherapy including patients who are relatively younger and without antecedent hematological disorders or complex cytogenetics. No standard of care regarding less intensive therapy has been established in these patients. Hematopoietic growth factors are associated with more rapid recovery following aggressive chemotherapy but studies have not been uniform in demonstrating improved disease-free or overall survival in patients treated with growth factors either during or following chemotherapy. In contrast, good outcomes have been demonstrated in older patients treated with standard therapy for acute promyelocytic leukemia, when they are able to tolerate aggressive chemotherapy.
High dose chemotherapy with autologous stem cell rescue has resulted in durable responses in a subset of elderly patients with AML. However, results are biased by the relatively small fraction of patients eligible for transplant due to comorbidities and the need to demonstrate stable responses to standard chemotherapy prior to pursuing autologous transplant. Allogeneic transplantation is associated with lower relapse rates due to the graft versus disease effect mediated by allogeneic lymphocytes. In an effort to increase the accessibility of allogeneic transplant to older patients and minimize treatment-related morbidity and mortality, reduced intensity transplant conditioning has been explored. This has resulted in decreased risk of regimen related toxicity and may decrease risk of graft versus host disease by decreasing inflammatory mediators. However, graft versus host disease remains a major concern particularly in older patients who demonstrate increased risk for this complication. Despite the concerns for toxicity, allogeneic transplantation particularly with reduced intensity conditioning is likely the only potentially curative option for many patients with poor risk AML. Appropriate selection of candidates is crucial. Of note, reduced intensity transplantation is most effective in low disease states, where the cell mediated effects have a chance to develop prior to disease progression.
Gemtuzumab ozogamicin consists of an antibody directed against the myeloid CD33 antigen bound to a chemical toxin colicomicin. It has been explored as therapy for elderly patients with recurrent AML. Fifteen percent of patients demonstrated evidence of complete remission and an additional 11% exhibited resolution of marrow leukemia with incomplete recovery of platelets. There is no evidence that gemtuzumab is more effective than standard induction for initial therapy. There is conflicting data regarding the efficacy of multi-drug resistance inhibitors in conjunction with chemotherapy. While one study demonstrated improved outcomes when cyclosporine A was included in the treatment regimen, other studies have failed to confirm this, and other agents such as PSC-833 have not shown efficacy in randomized trials. Farnesyl transferase inhibitors have demonstrated encouraging biological effects with significant responses seen in a small minority of patients with refractory disease. They are currently being examined in combination with standard chemotherapies. Inhibitors of DNA methylation such as 5-azacytidine or decitabine have demonstrated efficacy in patients with myelodysplastic syndrome. Their use is currently being examined in older patients with AML. Clofarabine is a novel agent that inhibits DNA polymerases and ribonucleotide reductase. A phase I-II study examined the toxicity of efficacy of a 5-day course of clofarabine in combination with cytarabine 1 gm/m2 in patients with relapsed or refractory acute leukemia, including 25 patients with AML. Twenty-two and 16% of patients achieved CR and CRp (CR with incomplete platelet recovery), respectively.
Summary
Standard therapy for elderly patients with AML is inadequate. Efficacy of therapy is limited by poor tolerance of therapy and resistant intrinsic disease biology. Aggressive chemotherapy may have a role in patients with good prognostic factors. Selected cohorts of patients may benefit from allogeneic transplantation with RIC. Novel agents targeting biological pathways are being explored alone or in combination in an effort to improve therapeutic options for this population.