Course Authors
Frederick Sweet, Ph.D.
Dr. Sweet is Professor of Reproductive Biology in Obstetrics and Gynecology, Washington University School of Medicine, St. Louis, Missouri.
Dr. Sweet reports no commercial conflicts of interest.
Estimated course time: 1 hour(s).

Albert Einstein College of Medicine – Montefiore Medical Center designates this enduring material activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
In support of improving patient care, this activity has been planned and implemented by Albert Einstein College of Medicine-Montefiore Medical Center and InterMDnet. Albert Einstein College of Medicine – Montefiore Medical Center is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
Upon completion of this Cyberounds®, you should be able to:
Discuss the history and derivation of modern medical ethics
Trace the twists and turns of Hippocrates' traditional ethics through the 20th century
Discuss the controversial patient care and biomedical research issues facing today's physicians and researchers.
Definition of Medical Ethics
"The principles of proper professional conduct concerning the rights and duties of the physician, patients, and fellow practitioners, as well as the physician's actions in the care of patients and in relations with their families."
http://cancerweb.ncl.ac.uk/cgi-bin/omd?medical+ethics
-- According to the On-Line Medical Dictionary
Published at the Dept. of Medical Oncology
University of Newcastle upon Tyne
[accessed 41,771,900 times]
Author's Operating Hypothesis
Laws contain the codification of the minimum community standards set down by legislative bodies, reflecting a consensus of behavioral standards set by the community at large. As such, the law represents a minimal set of standards that, if violated, provide for penalties, prescribed by legislators. However, medical ethics constitute a set of standards that are higher than the legal standards. They are set by members of the medical profession, based on the medical community's standards for the professional conduct of its members. Accordingly, medical ethics embody higher standards than legal standards -- or at least they ought to.
Early Medical Ethics: Hippocrates' Oath
The classical medical oath by Hippocrates can be found at the Public Broadcasting System's (PBS) Web site: http://www.pbs.org/wgbh/nova/doctors/oath_classical.html
This site is permanently maintained in conjunction with its four-part NOVA doctors series produced by Michael Barnes. The PBS site contains numerous responses by practicing physicians under Doctors' Responses and by the public under Non-Doctors' Responses. Additionally, PBS provides many links to discussions on the pros and cons of the Hippocratic Oath. See also, PBS's Survivor M.D. Site Map at: http://www.pbs.org/wgbh/nova/doctors/textindex.html.
The first recorded administration of the Hippocratic Oath in a medical school was at the University of Wittenberg in Germany in 1508.(1) Yet, the oath did not become a standard part of formal medical school graduation ceremonies until 1804, when it was incorporated into the commencement exercises at Montpellier, France.(3) Thereafter, during the 19th century this custom spread to both sides of the Atlantic Ocean. However, well into the 20th century, relatively few American physicians had formally taken this oath. In 1928, according to a survey by the Association of American Medical Colleges, only 19 percent of medical schools in North America included the oath in their commencement exercises.(4)
Hippocrates, an ancient Greek physician, probably lived between 460 and 380 B.C.

Figure 1. Hippocrate Refusant Les Presents D'Artaxerces (1792).

Anne Louis Girodet de Roussy (1767-1824)
While Hippocrates (Khios, Greece) is seated, D'Artaxerces is pouring money at his feet. Courtesy, National Library of Medicine.
Interestingly, the oath bearing Hippocrates' named is at the same time one of the most revered and yet misunderstood words in the history of medicine.(1) It is often misquoted. For example, the well known phrase, "First, do no harm" (translated into Latin as Primum non nocere), is mistakenly ascribed to Hippocrates' oath despite the fact that it doesn't appear anywhere in the pledge ascribed to him. Rather, Hippocrates came closest to issuing this directive among his writings in Epidemics, "As to diseases, make a habit of two things -- to help, or at least, to do no harm."(1)
The differences between the promises made in the original version of Hippocrates' oath and the oaths sworn today are nearly unrecognizable. The most obvious example is that few, if any of us, still believe in the ancient Greek gods Apollo, Asclepius, Hygieia and Panaceia. Therefore, we no longer pledge allegiance to them. By contrast, today, spirituality in general has little connection with medical science. In 1993, a content analysis of the oaths administered at 147 U.S. and Canadian medical schools revealed that only 11 percent of the various forms of the Hippocratic Oath invoked a deity.(5)
Today, nearly every U.S. medical school administers some form of professional oath to its some 16,000 men and women eager to receive their medical degrees. However, Hippocrates would not recognize most of the pledges ascribed to him. This revisionism is not unique to our time. In fact, alterations of the Hippocrates' oath began soon after its first recitation, generally reflecting changing values, customs and beliefs associated with medical ethics.
Two controversial vows in the original oath formulated by Hippocrates still divide many medical doctors: the pledges never to participate in euthanasia and abortion.(1),(2) These prohibitions had applied primarily to those identified as Hippocratic physicians, a medical sect representing a relatively small minority of all self-proclaimed healers. The early refusal to participate in euthanasia may have been based on philosophical or moral beliefs in preserving the sanctity of life or simply on their wish to avoid involvement in any act of assisted suicide, murder or manslaughter.
Reliable historical documents record that ancient Greek and Roman physicians were confronted with terminally ill patients who preferred a quick, painless death by means of poison rather than letting nature take its course.(2) There certainly were no laws in the ancient world against suicide. Indeed, it was fairly common for physicians to recommend this "option" to a patient with an incurable disease.
In both the ancient Greek and the Roman Empire, abortion (typically effected by means of a pessary to induce premature labor) was practiced as commonly as euthanasia. But later, in predominantly Christian countries, especially the oaths written during the Middle Ages revised the Hippocratic Oath to prohibit abortion. Today, the debate over euthanasia and abortion continues, although the relevant sections of Hippocrates' oath are simply omitted from most oaths administered by U.S. medical schools. As of 1993, only 14 percent of medical school oaths had prohibited euthanasia and only 8 percent prohibited abortion.(5)
Nazi Medicine: Rise of a New Ethos
After 1933, Nazis, including Hitler himself, expressed great admiration for the American eugenics movement, soon modeling their own sterilization laws and programs on earlier ones that had first been launched in the United States. Indeed, state-sanctioned sterilization of approximately 60,000 Americans started with a law passed in Indiana in 1907 that spread throughout the country, with similar laws ultimately enacted in 28 other states. Virtually all of these sterilization procedures had been conducted with limited or no informed consent.(7)
The early eugenics movement in America that began in Cold Spring Harbor(8) played an important role in the passage of an immigration law of 1924.(9) Its eugenic screening criteria and arbitrary immigration quotas had been based on the 1890 U.S. census figures, specifically designed to limit immigration from Eastern Europe because these people were considered to be hereditarily inferior.
[NB: More comprehensive discussions on the history and court cases associated with both the U.S. Public Health Service and also America's and Nazi Germany's eugenics movements are provided by Prof. Maxwell J. Mehlman in his recent Health Law/Bioethics Cyberounds entitled, "The Dark Side of Public Health".]
By 1938, the 1924 America immigration law had doomed thousands of East Europeans fleeing Nazi persecution by denying them entry into the United States. Perhaps the American eugenics movement began as a well-intentioned use of science for improving the human condition, but it very rapidly devolved into racism (in the guise of science) and led directly to deadly public policy in Nazi Germany.(7),(9)
Nazi propaganda had been specifically designed to limit the German people's feelings of sympathy and empathy for victims of their atrocities. The Jews and other untermenschen were characterized as inferior beings, not worthy of sympathy and empathy because they were threats to the Aryan race and Germany.(10) However, Robert Proctor, perusing official records and medical journals in Germany from the 1930s and 40s, discovered that some 75% of German physicians (and a similar percentage of German attorneys) had joined the Nazi Party.(11) This was a startling statistic given that not more than 15% of ordinary German workers, on behalf of whom Hitler's party had supposedly been organized, were Nazi Party members. One is left to presume Nazi physicians had been motivated to subvert their Hippocratic Oaths in order to build lucrative careers under the Third Reich rather than because of propaganda and fanatical ideology.
In the early days of the Third Reich, Nazi medicine focused on improving the Aryan German "race" by selectively weeding out those who had a congenital birth defect, were feeble minded or even had suffered a permanent injury thorough an accident. It would be the latter group of wounded German soldiers and their families who eventually put a stop to the "applied eugenics" being carried out at a hospital in Hadamar, Germany.
Killing Hospital at Hadamar: Prelude to Death Camps
In 1906, the Korrigenden-Anstalt in Hadamar had been established as a mental institution. By 1930, the institution could accomodate 320 patients. However, as required by the new Nazi laws, the nursing costs at Hadamar had to be reduced from 1934 onward. By 1936, Hadamar had become critically overcrowded and conditions worsened because of poor quality and reduced food rations. The buildings had originally been constructed to hold only 250 persons but by 1939 about 600 inmates were crowded in cramped quarters.
Figure 2. In 1983, the Hadamar Memorial Was Installed at the Infamous Building, Which, to This Day, Is Still Used as a Mental Institution.(13)

Photo courtesy of the Aktion Reinhard Camps team.
During late August 1939, patients were distributed to surrounding mental homes because Hadamar was now needed to serve as a military hospital. From November 1940 until January 1941, sickrooms were converted into quarters for personnel and administration staff of the new Hadamar euthanasia killing centre "T4."
[NB: The headquarters of the "euthanasia" operation were at Tiergartenstrasse 4 in Berlin and the code name for the program was derived from that address.]
Of the number of people killed in the T4 and similar programs in Nazi Germany, the following statistics are usually given: adult mental patients from institutions, 80,000 to 100,000; children in institutions, 5,000.(12) It has been estimated that, by the end of 1941, 3,521 'beds' had been emptied for other uses. About 70,000 patients had been gassed and over 20,000 had died through starvation and lethal medication, approximately one-third of the places for the mentally ill.(12) These operations, at first used for ridding Nazi Germany of its erbkranken (hereditary defectives), were developing a technology that set the stage for what rapidly evolved into the "final solution to the Jewish problem" that the world would later call the Holocaust.
Penalties for Practicing Nazi Medicine
After 1942, Nazi "medical" experiments were carried out by white coated physicians such as Josef Mengele and Carl Clauberg at the Buchenwald, Dachau and Auschwitz death camps.
Figure 3. A. Dr. Carl Clauberg, Ob & Gyn and B. Medical "Experiment" at Block 10 at Auschwitz.
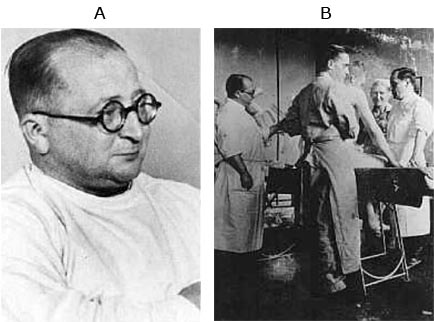
3A. Courtesy U. S. Holocaust Memorial Museum archives www.ushmm.org.
3B. Clauberg chose married women between the ages of twenty and forty, preferably those who had borne children. After returning to Germany from a Soviet prison camp in 1950, Clauberg would proudly claim, he had "perfected an absolutely new method of sterilization." Courtesy U. S. Holocaust Memorial Museum archives www.ushmm.org.
Below is a list of Nazi physicians who, after World War II had ended, were tried and convicted at the Nuremberg trial, and then executed by hanging in 1947. Their three most serious offenses were: war crimes, crimes against humanity, and membership in a criminal organization (i.e., the Nazi Party).(15)
Figure 4. Doctors' Trial in Nuremberg, 1947 and B. Witness Testifying at the Doctors' Trial in Nuremberg, 1947.
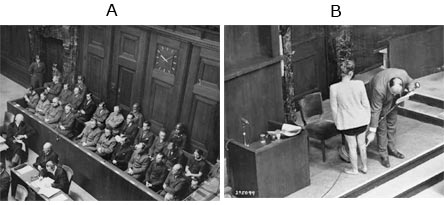
Courtesy of the U.S. Holocaust Memorial Museum archives, www.ushmm.org.
Figure 5. Nazi Doctors Sentenced to Death at Nuremberg.
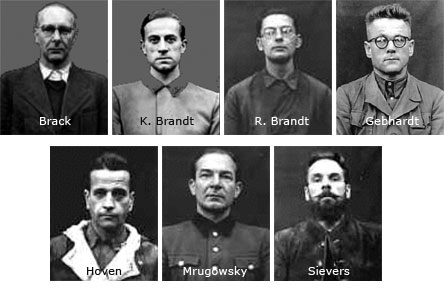
Dr. Viktor Brack, SS Oberf¨hrer (Senior Colonel), of the Euthanasia Program, Operation T4
Dr. Karl Brandt, Hitler's personal physician
Dr. Rudolf Brandt, Admin. Officer to organizer Himmler
Dr. Karl Gebhardt, personal physician to Himmler, president, German Red Cross
Dr. Waldemar Hoven, Chief Doctor of Buchenwald
Dr. Joachim Mrugowsky, Chief Hygienist of the Reich Physicians SS and Police, and of the Institute of the Waffen SS
Dr. Wolfram Sievers, Director of the Institute for Military Scientific Research, also Deputy Chairman of the Managing Board of Directors of the Reich Research Council
Courtesy of the U. S. Holocaust Memorial Museum archives, www.ushmm.org.
Figure 6. Sentences Carried Out following Doctors' Trial in Nuremberg (1947).

Courtesy of the U. S. Holocaust Memorial Museum archives, www.ushmm.org .
In passing, it is of historical interest to note that certain Nazi doctors convicted in Nuremberg of somewhat lesser war crimes (or acquitted for lack of sufficient evidence) were secretly brought to the United States and given jobs on military bases supervising medical experiments.(19) The importation into America of Nazi doctors was through a program named Project (aka Operation) Paperclip, implemented by the then newly formed Central Intelligence Agency.
Among the scores of Project Paperclip Nazi doctors were: Hermann Becker-Freyseng (Captain of Medical Services of the Air Force and Chief of the Department for Aviation Medicine of the Chief of Medical Services of the Luftwaffe, convicted) and Konrad Schaefer (Doctor on the Staff of the Institute for Aviation Medicine, acquitted).(18)
Figure 7. Project Paperclip.
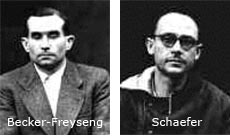
Dr. Hermann Becker-Freyseng, Capt. Medical Services Luftwaffe, Chief of the Department for Aviation Medicine
Dr. Konrad Schaefer, Staff Doctor of the Institute for Aviation Medicine, Berlin
Figure 8. High Altitude and Freezing Experiments.
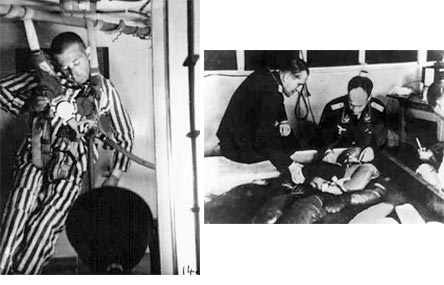
High altitude (left) and freezing (right) experiments were conducted at the Dachau concentration camp for the Luftwaffe (Air Force) from March until August 1942.
Courtesy of the U. S. Holocaust Memorial Museum archives, www.ushmm.org.
Along with another notorious Nazi doctor, Hubertus Strughold,(19) Brecker-Freyseng and Schaefer continued their high altitude decompression experiments for the U.S. Air Force (on American soil) that they had begun several years earlier on concentration camp inmates in Germany. However, now American military volunteers were used with their informed consent and it was forbidden to keep them in the decompression chambers to the point of death.
The Nuremberg Code of 1947 is considered by many to be the most important document in the history of medical research.(20) The Code was formulated by American judges following the trials of Nazi physicians convicted of heinous experiments on humans in concentration camps. Atrocities committed in the name of medicine during World War II, examined during the Nazi Doctors' Trials in Nuremberg in 1946, would ultimately lead, during the succeeding decades, to a growing interest in bioethics. After the conclusion of the Nuremberg Doctors' Trial, the recitation of an oath at American medical school graduation ceremonies became an increasingly important component.(5)
The 1947 Nuremberg Code is essentially a list of 10 specific standards for the conduct of medical experiments.(20) These standards have been extended to the practice of medicine generally and are now considered the "Ten Commandments" of ethical conduct for modern medical research on human subjects:
- The voluntary consent of the human subject is absolutely essential. [NB: Today, this is elaborated as "informed consent"]
- The experiment should be such as to yield fruitful results for the good of society, unprocurable by other methods or means of study, and not random and unnecessary in nature.
- The experiment should be so designed and based on the results of animal experimentation and a knowledge of the natural history of the disease or other problem under study that the anticipated results justify the performance of the experiment.
- The experiment should be so conducted as to avoid all unnecessary physical and mental suffering and injury.
- No experiment should be conducted where there is an a priori reason to believe that death or disabling injury will occur; except, perhaps, in those experiments where the experimental physicians also serve as subjects.
- The degree of risk to be taken should never exceed that determined by the humanitarian importance of the problem to be solved by the experiment.
- Proper preparations should be made and adequate facilities provided to protect the experimental subject against even remote possibilities of injury, disability or death.
- The experiment should be conducted only by scientifically qualified persons. The highest degree of skill and care should be required through all stages of the experiment of those who conduct or engage in the experiment.
- During the course of the experiment the human subject should be at liberty to bring the experiment to an end if he has reached the physical or mental state where continuation of the experiment seems to him to be impossible.
- During the course of the experiment the scientist in charge must be prepared to terminate the experiment at any stage, if he has probable cause to believe, in the exercise of the good faith, superior skill and careful judgment required of him, that a continuation of the experiment is likely to result in injury, disability, or death to the experimental subject.
Tuskegee Syphilis Experiment
"The United States government did something that was wrong -- deeply, profoundly, morally wrong. It was an outrage to our commitment to integrity and equality for all our citizens... clearly racist."
-- President Bill Clinton's apology to eight remaining survivors of the Tuskegee Syphilis Experiment
May 16, 1997
Between 1932 and 1972, the U.S. Public Health Service (USPHS) carried out a long-term experiment on 399 African American men in the late stages of syphilis. These men were for the most part illiterate sharecroppers from one of the poorest counties in Alabama. They had never been told what disease they were suffering from or of its seriousness. Informed that they were being treated for "bad blood", their doctors had no plans to cure them of syphilis.(21) Indeed, the doctors never had any intention of making the men better, even though Ehrlich's Salvarsan treatment for syphilis had been around for some 22 years(22) when the Tuskegee experiment was begun in 1932 and the cure for syphilis, antibiotics, had existed for at least 25 years when the experiment was forcibly stopped. Meanwhile, the Nuremberg Doctors Trial had ended more than 25 years earlier.
The underlying hypothesis being tested was that white humans experience more neurological complications from syphilis than blacks but that blacks are more susceptible to cardiovascular damage than whites. Yet it had never been made clear exactly how confirming these suppositions would have changed the clinical treatment of syphilis for anyone.(21)
To be sure that the men would show up for a painful and potentially dangerous spinal tap, USPHS doctors misled them with a letter full of promotional hype: "Last Chance for Special Free Treatment." That autopsies would eventually have to be performed on them was also concealed.
The data for the experiment were to be collected from autopsies of the men. Thus they were deliberately left to degenerate under the ravages of tertiary syphilis -- which commonly includes tumors, heart disease, paralysis, blindness, insanity and death. "As I see it," one of the doctors involved explained, "we have no further interest in these patients until they die."(21)
When in 1972 the experiment was finally stopped, 28 of the men had died directly of syphilis, 100 were dead of related complications, 40 of their wives had been infected and 19 of their children had been born with congenital syphilis. How had these men been induced to endure a fatal disease in the name of science?
Perhaps the most disturbing aspect of the experiment was how zealously the USPHS kept the syphilitic men from receiving treatment. Indeed, even though several nationwide campaigns to eradicate venereal disease came to Macon County, the men were prevented from participating. When penicillin -- the first real cure for syphilis -- was discovered in the 1940s, the Tuskegee men were kept from receiving the medication.
On July 25, 1972, the Washington Star finally broke the Tuskegee syphilis story in an article by Jean Heller of the Associated Press. Her source was Peter Buxtun, a former USPHS venereal disease interviewer, one of the few whistle blowers during all of those years. The unrepentant USPHS, however, claimed that the men had been "volunteers" and "were always happy to see the doctors." An Alabama state health official who had been involved in the project claimed, "somebody is trying to make a mountain out of a molehill."
Borgna Brunner concludes, "Who could imagine the government, all the way up to the Surgeon General of the United States, deliberately allowing a group of its citizens to die from a terrible disease for the sake of an ill-conceived experiment? In light of this and many other shameful episodes in our history, African Americans' widespread mistrust of the government and white society in general should not be a surprise to anyone."(21)
Tuskegee Post Mortem -- A Return to Slavery?
Professor B. Roy argues that the central issue of the Tuskegee Syphilis Experiment had been property. That is, property in the subjects' bodies and intellectual property.(24)
Once removed from the body, tissues and bodily fluids were not legally the property of the Tuskegee subjects. Consequently, there was not a direct relationship between a patient and research that used this sera. The U.S. Public Health Service was free to exercise its property right in Tuskegee sera for developing serologic tests for syphilis with commercial potential.
To camouflage the true meaning, the USPHS made a distinction between direct clinical studies and indirect studies of tissue and body fluids. This deception caused all reviews, to date, to limit their examination to documents labeled by the USPHS as directly related to the Tuskegee Syphilis Experiment. This excluded other information in the public domain. Despite the absence of a clinical protocol, this subterfuge led each reviewer to conclude falsely that the Tuskagee Syphilis Experiment was a clinical study.
Based on publications of indirect research using sera and cerebrospinal fluid, a recent article by Roy reveals a further very dark history of the Tuskegee Syphilis Experiment.(24) Syphilis can only be cultivated in living beings. As in slavery, the generative ability of the body made the Tuskegee subjects real property, investing the sera of these subjects with immense commercial value for untreated syphilis. Published protocols exploited the Tuskegee Syphilis Experiment to invent and commercialize biotechnology for the applied science of syphilis serology.
U.S. Army Medical Experiments
Three years after the Tuskegee Syphilis Experiment was terminated, congressional inquiries were conducted by the Senate Select Committee on Intelligence Activities and joint hearings by the Senate's Labor and Public Welfare Committee and the Judiciary Committee during 1975 and 1976. Although the congressional investigations were not related to the clearly unethical medical experiments earlier performed on the unsuspecting African American syphilitics, in more than one sense something was in the air.
Taylor and Johnson prepared a report on the use of volunteers in chemical agent research and wrote, "This report was the result of a request to the Inspector General and Auditor General of the Department of the Army (DoA) by the Secretary of the Army to research the use and treatment of human volunteers in chemical agent research."(25) The Army was responding to individual Members of Congress, private citizens and the press regarding the use of human volunteers in testing of hallucinogenic substances in DoA chemical warfare research.
Figure 9. Declassified MKULTRA Document.
The report focused largely on psychochemical testing programs and on testing programs from approximately 1950 to 1975. It also related certain specific aspects of the history of chemical warfare research in regard to treatment of human volunteers and general attitudes toward and compliance with the Nuremberg Codes of 1947.
Of course, there is not enough time and space here to even skim over the 420 pages of the report by Taylor and Johnson. But here is the gist of their conclusions: "The major conclusion was that the secrecy, applied to the projects, to the overall research program, and even to the official guidelines governing use of human volunteers, left ample room for misinterpretation, lack of knowledge about, and outright disregard for established policies and guidelines."(25)
The report continues: "In July 1950, research was placed under the control of the Army by the Organization of the Army Act. Despite the establishment in 1947 of the Nuremberg Codes regarding the appropriate use and treatment of human subjects in research, Taylor and Johnson reported that no documentation could be found about whether the Army was explicitly bound by the Codes. By 1952, the Armed Forces Medical Policy Council filed a request to use human subjects and suggested that the Nuremberg Codes be used as guidelines."
"By 1959, Secretary of the Army Brucker gave blanket approval for all projects utilizing 'non-lethal incapacitating agents,' and the period between 1959 and 1975 was typified by great inconsistency in policy and practices relating to research with human volunteers. The situation became so bad, and the outcry from Congress, the press, and the citizenry so intense, that all research with human volunteers was suspended in 1975 by Acting Secretary of the Army Norman Augustine."
Then the report reiterates the Ten Commandments of medical ethics, "Key Elements of the Nuremberg Code of 1947," as something of a prayer.
A U.S. Senate committee chaired by Senator Frank Church (D-ID) in 1975 (The Church Committee) had, in fact, been the United States Senate Select Committee to Study Governmental Operations with Respect to Intelligence Activities. A precursor to the U.S. Senate Select Committee on Intelligence, the Church Committee investigated intelligence gathering by the CIA and FBI for illegal activities.
On the Senate floor in 1977, Senator Ted Kennedy (D-MA), a Committee member, said:
"The Deputy Director of the CIA revealed that over thirty universities and institutions were involved in an 'extensive testing and experimentation' program which included covert drug tests on unwitting citizens 'at all social levels, high and low, native Americans and foreign.' Several of these tests involved the administration of LSD to 'unwitting subjects in social situations.' At least one death, that of Dr. Olson, resulted from these activities. The Agency itself acknowledged that these tests made little scientific sense. The agents doing the monitoring were not qualified scientific observers."(26)
Contemporary Controversial Medical Experiments
Medical ethical standards are not static, as newspaper headlines continue to remind us. Thus a new national research project in emergency medicine seeks to examine the treatment of certain patients without their prior consent.(27) A $50 million, five-year project will involve more than 20,000 patients at 11 sites in the United States and Canada and it is designed to improve treatment after accidents, shootings, cardiac arrests and other emergencies.
According to the lead sentence, "The federal government is undertaking the most ambitious set of studies ever mounted under a controversial arrangement that allows researchers to conduct some kinds of medical experiments without first getting the patient's permission." Organizers of the three studies say this project will offer an unprecedented opportunity to find better ways to resuscitate people whose hearts suddenly stop, to stabilize patients who go into shock and to minimize damage from head injuries.
Although many trauma specialists and some bioethicists had endorsed the project, others question it. The research violates fundamental ethical principles say the harshest critics.
The first experiments will involve nearly 6,000 patients, treating patients who are in shock or have suffered head injuries from a crash, fall, or some other trauma. Each year, some 40,000 such patients show up at hospitals where the standard practice is to give them saline infusions to stabilize their blood pressure.
The study will involve emergency medical workers randomly infusing some patients with solutions containing much higher levels of sodium, with or without Dextran. Preliminary results from research with animals, and some small studies involving people, have shown that hypertonic solutions can save more lives and minimize brain damage.
Another somewhat similar experiment will involve about 15,000 patients. This experiment is designed to determine how best to revive patients whose hearts suddenly stop beating. About 180,000 Americans suffer such sudden cardiac arrests each year.
Rejecting the position that a patient brought into an emergency room need not give informed consent, George J. Annas, a bioethicist at Boston University recently said, "This just seems like lazy investigators not wanting to try to get informed consent in situations where it is difficult to get it, so they say it is impossible. I don't think we should use people like this."
Yet others are concerned that patients may receive experimental therapies that could turn out to be inferior to standard treatments.
However, Myron Weisfeldt of the Johns Hopkins University School of Medicine, who is overseeing the project said, "We will never know the best way to treat people unless we do this research. And the only way we can do this research, since the person is unconscious, is without [their] consent."(27)
Human Stem Cell Jihad
A persistent medical ethical controversy continues to hang over human stem cell research.
Ever since it was recognized that political capital could be harvested from the abortion issue, first by Jimmy Carter(28) and subsequently by the Reagan-Bush administration, any research on human embryos at any stage of development has become grist for this political mill. More recently, George W. Bush, who inherited the human embryo issue and, proud of his so-called conservative political base that included pro-natal and pro-embryo supporters, continued this politicization. Though there is not enough paper to write on nor enough electromagnetic ether available to do justice to the contraception-abortion-embryo issue with respect to morality, science and ethics go, with this caveat, we will, nevertheless, try to say something about the science and ethical arguments involved.
Stem cells are primal cells that exist in all multi-cellular organisms. They retain the ability to renew themselves through mitotic cell division, and they can differentiate into a diverse range of specialized cell types. The medical research in the field of human stem cells developed after the work of Canadian scientists Ernest A. McCulloch and James E. Till in the 1960s.(29)
There are three broad categories of mammalian stem cells: the embryonic stem cells from blastocysts, adult stem cells from adult tissues and cord blood stem cells from the umbilical cord. In a developing embryo, stem cells can differentiate into all of the specialized embryonic tissues. In adult organisms, stem cells and progenitor cells act as a repair system by replenishing specialized cells in the body.
The use of stem cells in medical therapies has been proposed because through cell culture they can be grown and transformed into specialized cells with the characteristics of the cells in various tissues such as muscles or nerves. In particular, embryonic cell lines (autologous embryonic stem cells generated through therapeutic cloning) and the highly plastic adult stem cells from umbilical cord blood or bone marrow have been touted as promising candidates.(30)
Figure 10. Harvesting Human Embryonic Stem Cells
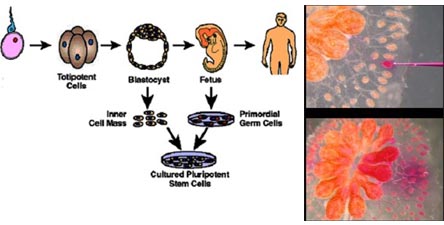
Harvesting human embryonic stem cells (left), visible only under a microscope (right), for culturing pluripotent stem cells. Courtesy, National Library of Medicine.
It seems self-evident that the reason human blastocycsts are the best candidates for ultimately generating highly differentiated tissues is that cells produced by the first few divisions of the fertilized egg are totipotent. These cells can differentiate into embryonic and extraembryonic cell types. Of course, these totipotent cells are at the center of the political debate because they are derived from fertilized -- sperm + egg -- cells. "Pro-natal, pro-embryo" supporters are prepared to do whatever it takes to prevent government funding of medical research that disturbs the fertilized human egg.
Unfortunately, pro-natal, pro-embryo supporters seriously compare stem cell research to the subjects of Nazi medical research -- fully formed humans -- making it difficult to engage in an impartial medical ethical debate. So far as neurobiologists can tell, however, a cluster of 64 or 128 human cells can feel no pain. After all, they are not yet differentiated into nerve or other tissues and thus no pain can be felt. Indeed, the main stem cell debate centers on religious arguments having to do with when humans acquire a soul. Trying to reach some common ground with someone who insists that a small, nearly invisible cluster of human cells is virtually a pre-college graduate cannot lead to compromise. That is why resolving the stem cell controversy, clearly, comes down to political power and not carefully researched scientific or philosophical arguments.
Did Hippocrates have to face similar medical ethical issues?