Course Authors
Peter Barland, M.D.
Release Date: 10/05/1996
Upon completion of this Cyberounds®, you should be able to:
The examination of synovial fluid obtained by needle aspiration is a critical step in the evaluation and treatment of many patients with acute arthritis. The recent availability of PCR analysis offers the primary care physician a sensitive test for the causative infectious agents of gonococcal arthritis and Lyme disease.
In this Cyberounds®, we will illustrate how to aspirate the elbow and the knee and discuss the principles of synovial fluid examination.
Purpose of Joint Aspiration
The primary reason for aspirating a joint is to rule out the possibility of infectious arthritis which, if incorrectly treated, can damage a joint irreversibly. In addition, both gout and pseudogout can only be diagnosed with certainty through the examination of synovial fluid. Joint aspiration may also be useful therapeutically by relieving the pain caused by a distended synovial capsule or by the removal of blood from the joint space. Re-aspiration of infected joints not only removes WBC's and protelolytic enzymes from the joint, but it may be helpful in judging the response to treatment.
Indications for Joint Aspiration
Joint aspiration is indicated in all patients with:
- Acute monarthritis and fever
- First attack of acute monarthritis
- Monarthritis in an immunocompromised host
- Rheumatoid arthritis and a monarticular flare.
Joint aspiration is indicated in most patients with:
- Chronic monarticular arthritis with a large effusion
- Chronic monarticular arthritis with pain at rest.
Techniqute of Joint Aspiration
Ideally, joint aspiration should be done before treatment with antibiotics is initiated. However, in patients with suspected cellulitis overlying the joint to be aspirated, it is preferable to have the patient on antibiotic therapy first, so as to avoid the possibility of introducing infectious organisms into the joint space. It is not necessary to routinely obtain an x-ray of the joint prior to aspiration.
It is appropriate for the primary care physician to aspirate the knee, wrist, elbow, and shoulder joints, as well as the olecranon and prepatellar bursae. The hip, sacroiliac, sternoclavicular, temporamandibular and subtalar joints should only be aspirated by physicians with special training, such as rheumatologists and orthopedists.
Before attempting to aspirate a joint, ascertain that the patient is not on anticoagulant therapy and does not have a clinically significant bleeding disorder. The skin over the joint should be cleaned with iodine or betadine. Then the skin and subcutaneous tissue should be anesthetized with 1-2% lidocaine or xylocaine, but the joint itself should not be infiltrated with anesthetic, as these contain antibacterial substances which can inhibit the growth of infectious agents that we're trying to culture and identify.
A 21-gauge needle is usually sufficient for most aspirations, though some fluids require a larger bore needle such as 19-gauge. It is important to adhere to the usual aseptic measures. Fluid should be aliquoted to an anticoagulated tube for cell count and crystal examination, to a sterile anticoagulated tube for culture and gram stain, and to a non-anticoagulated tube for chemical determinations (glucose and LDH). Testing synovial fluid for complement levels is of little value. Assays for rheumatoid factor, antinuclear antibodies, anti-Lyme antibodies and acute phase reactants are inappropriate.
The anatomical landmarks and direction of the needle are discussed below.
Figure 1. Anatomical Landmarks for Joint Aspirations.
A. The Knee
The knee may be aspirated from either the medial or lateral aspects. It is usually easier to tap when the joint is flexed approximately 20 degrees. The key landmark is the superior border of the patella and the angle of needle is almost parallel to the undersurface of the patella. Aspirating the suprapatellar bursa is often difficult since the needle often becomes obstructed by synovial tissue.
B. The Elbow
The needle enters the palpable space between the lateral epicondyle of the humerus and the olecranon process of the ulna. The needle will then be perpendicular to the long axis of the humerus.
The wrist should only be aspirated from the dorsal aspect - preferably with the joint flexed to approximately 20 degrees. A convenient landmark is the radial styloid with the joint space being AfAE?A?'Af†Ac€??cAfAE?Ac€ Af?cAc‚¬Ac„?cAfAE?A?'Af‚A??cAfAE?A??cAf?cAc‚¬A??!Af‚A?¬AfAE?Ac€¦Af‚A??!AfAE?A?'Af†Ac€??cAfAE?A??cAf?cAc€A!A?¬Af…A??!AfAE?A?'Af?cAc‚¬A??!AfAE?Ac€A!Af‚A?? 1/2 inch proximal to the tip of the styloid. I usually aim the needle perpendicular to and on the ulnar side of the extensor tendon of the second finger.
The ankle should be slightly plantar flexed and the needle should enter the joint 1/2 inch proximal to the tip of the medial malleolus and just lateral to the extensor tendon of the first toe. The needle should be directed distally towards the calcaneus.
THe prepatellar and olecranon bursae are very superficial structures which do not communicate with the knee and elbow joints. They can be easily aspirated using fluctuance as a guide.
Examination of Synovial Fluid
A great deal of important information can be learned from very simple tests of the synovial fluid. The color, clarity and viscosity of the fluid should be noted. Normal synovial fluid is usually colorless, clear and very viscous. Normal appearing fluid may be seen in the joint effusions caused by chronic osteoarthritis, hypothyroidism, acromegaly, amyloidosis and pulmonary hypertrophic osteoarthropathy. Fluid from patients with chronic inflammatory noninfectious arthritis usually is pale yellow due to the increased protein content, slightly cloudy due to the presence of WBC's and synovial lining cells and has a decreased viscosity. Fluid from infected joints usually is pale yellow, very cloudy or opaque and has a low viscosity. Fluid from an acute crystal arthritis can resemble either of the latter two fluids.
Bloody or serosanguinous fluid is usually found after major joint trauma, minor joint trauma in patients on anticoagulation therapy or with an acquired or inherited bleeding diathesis, occasionally in crystal synovitis and in the rare primary and metastatic tumors of the synovium. Chlylous or milky synovial fluid is occasionally seen in rheumatoid arthritis.
To judge the clarity of the fluid it is helpful to hold a tube of the unspun fluid in front of a typewritten page. Slightly cloudy fluid will reveal the print but is not clear enough to read through. Fluids with greater than approximately 25,000 WBC's per cubic milliliter will usually scatter light sufficiently so that the newsprint cannot be seen.
To judge viscosity, place a drop of the fluid between two fingers and see whether a string is formed from the fluid as the fingers are slowly separated.
Synovial fluid should also be examined for birefringent crystals, preferably using a polarizing microscope equipped with a built in compensator. However, you can use a light microscope (see below.) Uric acid crystals are negatively birefringent and therefore yellow when their long axis is parallel to the compensator, and needle shaped (Figure 2). Calcium pyrophosphate crystals, rhomboid in shape, are positively birefringent, and therefore blue when their long axis is parallel to the compensator. In order to be certain that the crystals are causing the synovitis they should be seen within a polymorphonuclear leucocyte (Figure 3). A third crystal -- basic calcium phosphate or hydroxyapatite may also cause an acute synovitis or bursitis. These crystals appear as amorphous material on both light and polarizing microscopy and require x-ray crystallography or special staining techniques for a definitive diagnosis. They may be suspected when soft tissue calcification of surrounding tendons and bursa are seen on x-ray.
Figure 2.
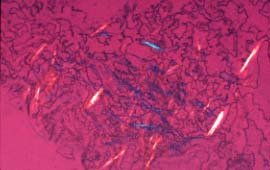
Synovial fluid with sodium urate crystals, polarized light with red compensator, microscopic.
Courtesy of Gower Medical Publishing Ltd.
Figure 3.
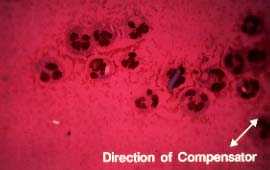
Synovial fluid with calcium pyrophosphate crystals inside PMN secondary to pseudogout.
Courtesy of Syntex
The WBC and differential WBC should be determined on all synovial fluids. A WBC >50,000/cubic milliliter with 90% polymorphonuclear leucocytes should be considered diagnostic of infection pending the results of the culture and antibiotic treatment started.
Synovial fluid should be sent for gram stain and culture. In addition to blood agar, the lab should culture the fluid under carbon dioxide for gonococci when indicated. Many laboratories now offer PCR analyses of synovial fluid for the rapid determination of suspected pathogens such as gonococci or Borrelia burgdorferi (for Lyme disease). The PCR technique is rapid and extremely sensitive--theoretically only a single proliferating organism is required, but the testing laboratory must be fastidious. Otherwise, specimen contamination will produce false positive results.
Common Mistakes and Misconceptions
- Withholding antibiotic treatment pending the results of the culture. In the appropriate setting, such as a sexually active female with a pustular skin rash, antibiotics should be started once the joint aspiration has been performed.
- Failure to culture fluid once intracellular crystals are seen. Infection and crystal arthritis can coexist since infection may cause release of crystals from insoluble deposits in the joint or may reduce the pH of the synovial fluid leading to the formation of crystals of either uric acid or calcium pyrophosphate.
- Not examining the fluid for crystals promptly. Calcium pyrophospate crystals may dissolve in fluid kept for many hours at room temperature. Uric acid crystals while more stable will also begin to dissolve after 24 hours at room temperature.
- Not examining the fluid crystals because a polarizing microscope is unavailable. Most crystals can be seen with a regular light microscope when the condenser is racked down to create a partial phase effect. Both uric acid and calcium pyrophosphate crystals appear lighter than the background under these conditions.