Course Authors
Gary M. Levin, M.D.
Release Date: 01/26/2005
Upon completion of this Cyberounds®, you should be able to:
Discuss pharmacologic treatments for glaucoma
Describe the mechanism of action of the latest eye medications
Discuss non invasive and laser treatments for glaucoma
Describe surgical interventions for glaucoma.
In Part I of this Cyberounds®, we discussed the evolution and refinement of glaucoma diagnosis as a consequence of new technologies such as ocular coherence tomography, corneal pachymetry and more sensitive visual field testing devices.
Similarly, with respect to glaucoma therapy, we have seen much progress in the pharmacologic and surgical treatments of the disease. Most significantly, the development of pharmacologic agents with fewer side effects has markedly improved compliance in patients with glaucoma.
Medical and Minimally Invasive Treatment
The Advanced Glaucoma Intervention Study, which began in 1994, has contributed much to the advances in early detection and more successful outcomes.(1)
Meiotic agents (drugs that cause papillary constriction) such as pilocarpine, physostigmine and phospholine iodide have largely been abandoned, replaced by prostaglandin agonists [bimataprost, latanaprost (Xalatan), travoprost (Travatan)] whose therapeutic mechanism of action increases uveoscleral outflow.(2),(3) Beta-blocking agents, e.g., timolol (Timoptic) are also used as first- or second-line drugs.(4) The beta-blockers act by decreasing aqueous production, increasing outflow and modifying blood flow to the eye.(5) The selective beta-blocking agents, e.g., betaxolol (Betoptic), although less likely to cause bothersome side effects, still have some risk of inducing problems in patients with bronchial disorders.
Oral carbonic acid anhydrase inhibitors acetazolamide (Diamox), methazolamide (Neptazane), have been replaced by topical carbonic acid anhydrase enzyme precursors such as dorzolamide hydrochloride (Trusopt) that can be applied directly to the eye as a drop. These agents pharmacologically block the enzyme carbonic acid anhydrase, which is crucial to aqueous humor production by the ciliary processes of the eye. Topical application of these agents has reduced side effects. (When administered systemically, these drugs can result in mood change and severe electrolyte disturbances.) Combination drugs incorporating prostaglandin agonists, carbonic acid anhydrase inhibitors and/or beta-blockers are now commonly used as well. (6),(7) The efficacy and duration of these drugs have been enhanced so that qd or bid dosage is often sufficient to maintain control.
It should be remembered that although these medications are given topically, there is some systemic absorption via the nasopharynx, and a topically applied beta-blocker or carbonic acid anhydrase inhibitor have been known to create depression, behavioral changes or other reactions. The prostaglandin agonists are usually given only once a day at bedtime. One of their physiologic effects is vascular dilation, causing a red eye, and there have been reported cases of iris color darkening(8) and hypertrichosis of the lashes.(9),(10),(11),(12)
Figure 1. Heterochromia of the Iris.

The left eye is normal, the right eye has hyperpigmentation of the iris. Hyperpigmentation, though not serious, is a common side effect of prostaglandin agonists. (Note: the left eye also has had a cataract removal. You can see a faint rim of lens capsule haze at 6'clock on the anterior surface of the pseudophacos).
The images were provided as a courtesy by images.md and are reproduced herein with permission for educational purposes only.
Therapeutic Agents Which May Interfere with Glaucoma treatment or Exacerbate Glaucoma
Background
Several different drugs have the potential to cause elevation of intraocular pressure (IOP). Two major pathophysiologic mechanisms by which elevated IOP can occur exist -- via an open-angle mechanism or via a closed-angle mechanism. Steroid-induced glaucoma is a form of open-angle glaucoma that usually is associated with topical steroid use but it may develop with oral, intravenous, inhaled or periocular steroid administration. Medications prescribed for a variety of systemic conditions (e.g., depression, allergies, Parkinson's Disease) can produce pupillary dilation and precipitate an attack of acute angle-closure glaucoma in anatomically predisposed eyes with narrow angles.
Open Angle
Drug-induced elevation of IOP is more common by an open-angle mechanism. Corticosteroids are a class of drugs that may produce IOP elevation by this mechanism. Not all patients taking corticosteroids will develop elevated IOP. Risk factors include preexisting primary open-angle glaucoma, a family history of glaucoma, high myopia, diabetes mellitus and history of connective tissue disease (especially rheumatoid arthritis).
Additionally, the number of people responding with an elevated IOP varies with the route of administration. More people respond from topically applied drops (including topically applied creams to the periorbital area). In order of decreasing frequency, incidence of elevated IOP is lower with intravenous, parenteral and inhaled routes of administration. Patients on chronic corticosteroid therapy can remain undiagnosed with an elevated IOP, which can result in glaucomatous optic nerve damage.
Steroid-induced IOP elevation typically occurs within a few weeks of beginning steroid therapy. In the majority of cases, the IOP lowers spontaneously to the baseline within a few weeks to months upon stopping the steroid. In rare instances, the IOP remains elevated. Additionally, there may be some patients whose underlying condition necessitates the continued use of corticosteroids despite the elevated IOP. These patients are treated identically to those with primary open-angle glaucoma.
Closed Angle
The majority of categories of drugs that list glaucoma as a contraindication or adverse effect are concerned with inducing an acute angle-closure glaucoma. These medications will incite an attack only in those individuals with occludable angles. The classes of medications that have the potential to induce angle closure are topical anticholinergic or sympathomimetic dilating drops, tricyclic antidepressants, monoamine oxidase inhibitors, antihistamines, antiparkinsonian drugs, antipsychotic medications and antispasmolytic agents. Sulfa containing medications may induce angle-closure glaucoma by a different angle-closure mechanism, involving anterior rotation of the ciliary body.(13)
Laser Treatments
Argon Laser Trabeculoplasty (ALT) is now being replaced by Selective Laser Trabeculoplasty (SLT).(14),(15) Both treatments focus laser energy on the trabecular meshwork overlying Schlem's canal, thereby increasing outflow of aqueous humor and thus lowering IOP. Because of its wavelength, Selective Laser Trabeculoplasty causes less injury to the meshwork.(16) ALT has been in use for more than 20 years and while not a permanent solution allows medical therapy to succeed in some cases for as long as eight years.(17) These treatments are applied through the transparent cornea with a special gonio lens.
Argon Laser photocoagulation is also applied in a panretinal pattern to the retina (with sparing of the macula) for patients who develop neovascularization of the iris and angle recess secondary to vein occlusion or other ischemic ocular syndromes. Neovascularization of the iris is manifest by ectropion uveae (hyperplasia of the iris pigment border) and fine vessels apparent on the anterior surface of the iris (rubeosis iridis).
Narrow Angle Gaucoma
The treatment of narrow or closed acute angle glaucoma requires a peripheral iridectomy, which can be created using either an argon thermal laser or a photodisruptive laser such as a YAG Laser. YAG Laser treatment is preferable and less traumatic in most cases. Thick irises may require applications of both laser types and, on rare occasions, as a result of poor visibility or other technical factors, a surgical iridotomy must be performed. The creation of an opening in the peripheral iris creates a direct outflow of aqueous humor to the angle recess, bypassing iris and/or papillary block.
Figure 2. Cross-sectional View of Iridotomy.
Anterior view of iridotomy visualized easily with reflex illumination by indirect ophthalmoscopy. Notice proximity of zonules between ciliary body and lens, allowing direct access of fluid from posterior chamber to angle recess and trabecular meshwork.
Figure 3. Iridotomy.
Artist's rendering of a patent iridotomy following YAG or argon laser iridotomy. This is performed under topical anesthesia at a slit lamp with a contact iridotomy laser lens.
About one-third of patients with angle closure problems will also develop chronic open angle glaucoma ("combined mechanism glaucoma"). These patients require further medical and/or surgical intervention eventually. Patients who have had iridotomy treatment for glaucoma must be followed regularly regardless of post iridotomy normal intraocular pressure.
Surgical Intervention
Indications
"Target intraocular pressure"(18) is defined as that pressure which results in non-progression of the visual field loss from glaucoma. In some cases, the target IOP may be 20 mm, 22 mm or 13 mm of mercury. If it is not possible to maintain this target IOP with multiple medications (or if patient compliance is poor) and when single or multiple laser Trabeculoplasty have also failed, a conventional filtering procedure is recommended.
The greatest challenge for our glaucoma patients, and for the treating ophthalmologist, is compliance. Numerous studies have shown that almost 50% of patients were non compliant despite being on only one medication. Surveys also show that glaucoma patients miss up to 100 days of treatment per year.(34) The problem is compounded by the fact that, on average, glaucoma patients usually have three additional ailments requiring prescription therapy - namely hypertension, arthritis and elevated cholesterol.
Table 1. Reasons for Non-Compliance.(34)
| Situational/Environmental factors | 49% (accountability, major life events, travel, away from home, competing activities, change in routine |
| Regimen factors | 32% (medication has too many side effects) |
| Patient factors | 16% |
| Provider factors | 3% (inadequate professional education) |
Conventional Filtering Procedures (CFP)
Filtering procedures can be divided into non-penetrating and penetrating.
Non-penetrating
Viscocanaliculostomy is a procedure used in Europe much more than the United States. This procedure involves placing an opening into the anterior chamber and then intubating Schlem's canal. Theoretically, this procedure allows the entire outflow drainage channels to continue to function.
Figure 4. Viscocanaliculostomy.

Viscocanalostomy is performed by a Grieshaber cannula. Healon G.V. (hyaluronic acid) is injected while slowly retracting the cannula.
Penetrating
Trabeculectomy or Trabeculectomy with Adjunctive Treatment
The classical filtering surgery involves developing a partial thickness, corneal-based scleral flap under which a trephination is made into the anterior chamber at Schlem's canal. The size and shape of the opening determine the end point of intraocular pressure control. The size is in the range of 0.5 mm. The area of the opening is loosely approximated with the hinged flap and covered anatomically with Tenon's capsule and conjunctiva.
Figure 5. Trabeculectomy.
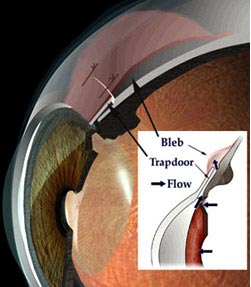
Artist's rendition in cross section.
Figure 6. Surgical Procedure -- Trabeculectomy.
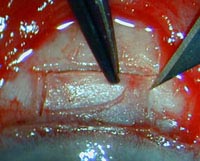
Sclerotomy flap measures about 4 mm in width, 0.3mm depth. Orientation: 12 o'clock at top of photo; grey zone is cornea limbus (anterior anatomic view at time of surgery).
Some surgeons utilize antimetabolites (5-fluorouracil or mitomycin) topically or by injection at or near the site of the trabeculectomy.(19) Each has its benefits and possible consequences.(20) 5-fluorouracil must be injected in the subconjunctival space at the time of surgery and regularly each week after surgery depending on the intraocular pressure and the appearance of the filtering bleb. Success rates, however, are improved using this adjunctive therapy. Mitomycin can be applied topically at the time of surgery at the site of the scleral flap. It may result, however, in a very thin avascular bleb, which enlarges, thins and may leak as time proceeds. However, these agents have increased the success rate of filtering procedures.(21),(22),(23)
Figure 7. Trabeculectomy -- One-Month Postoperatively.
The most frequent risks following filtering procedure are failure of the filter to form a functioning bleb and overfiltration resulting in ocular hypotension that, in turn, produces choroidal effusion and/or flat anterior chamber. In the early post-operative period, a loss of the anterior chamber can result in cataract, corneal edema and chronic angle closure.
The long-term risks from the filtering surgery include leaking of the filtering bleb and/or blebitis, a potential infection that can evolve into a blinding endophthalmitis.(24) All of these risks can be managed successfully with careful follow-up. These risks are much more common in patients who have had mitomycin as adjunctive treatment at the time of surgery. Some ophthalmologists prescribe a 4th generation quinolone topically once a day for the remainder of the patient's life to prevent the development of late blebitis and/or endophthalmitis.
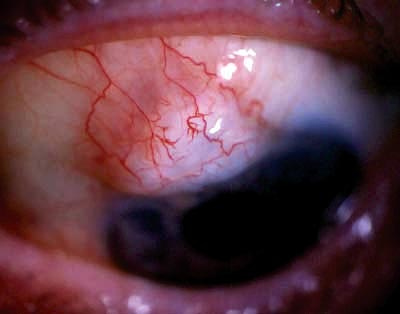
Figure 8. Blebitis.
Infection of the filtering bleb following trabeculectomy This can occur from one month to anytime post op.
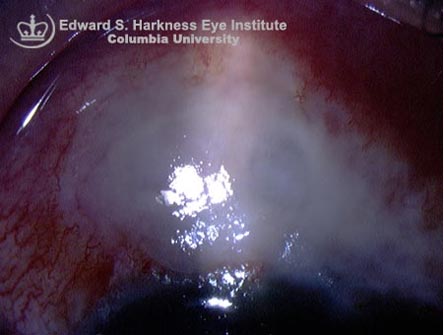
Figure 9. Endophthalmitis.

Endophthalmitis following a trabeculectomy. Notice the hazy cornea, circumcorneal hyperemia and the hypopyon (white blood cells) layered in the inferior anterior chamber.
Figure 10. Fluorescein Staining Secondary to 5-FU Toxicity to Corneal Epithelium.
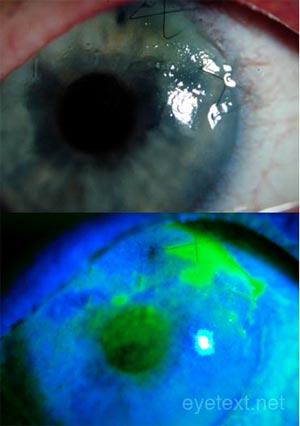
Figure 11. Thin Walled Filtering Blebs With Overfiltration.
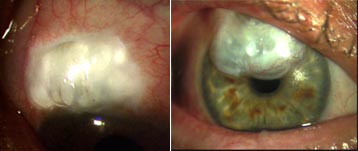
Thin walled filtering blebs with overfiltration secondary to topical adjunctive therapy with mitomycin at time of surgery. Significant risk factors are blebitis and endophthalmitis.(25)
Should several CFPs fail and/or in the presence of neovascular glaucoma an artificial shunt (see Figure 12) can be implanted. This procedure involves placement of an artificial tube into the anterior chamber via the angle recess, tunneled under the anterior cornea-scleral limbus into a reservoir device.
Figure 12. Tube Shunts.
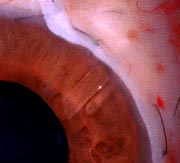
Note the clear tube in the anterior chamber, which connects with a reservoir under the edematous conjunctiva. This photo is one-week post-op.
Numerous devices have FDA approval and include the Baerveldt, Molteno, Krupin and Ahmed shunts.
Glaucoma drainage devices are an option in the management of complicated glaucomas that carry a high risk of failure from conventional filtering surgery.(26) Examples include the glaucomas associated with aphakia (absence of the lens) or pseudophakia, neovascular glaucoma, and glaucomas associated with trauma, uveitis, epithelial downgrowth, iridocorneal endothelial syndrome, vitreoretinal disorders and penetrating keratoplasty. Modifications in the various implant designs have been developed to limit the occurrence of postsurgical complications such as hypotony, serous and hemorrhagic choroidal detachment, tube and plate avulsion, tube exposure and corneal endothelial damage.(27)
Figure 13A and B. Reservoir Devices.
Figure 13A. Ahmed Valve.
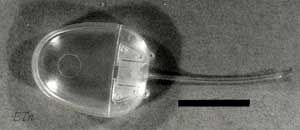
Figure 13B. Molteno Shunt.
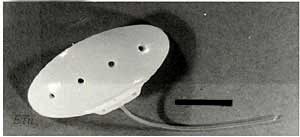
Figure 14. Other Aqueous Shunts and Reservoir Devices.
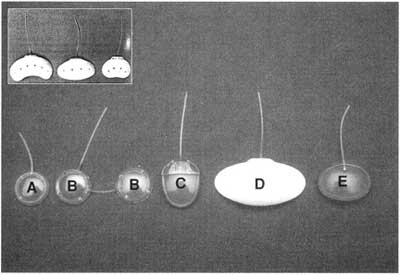
A. Baerveldt shut. B. Baerveldt shunt with two reservoirs. C. Ahmed Shunt. D. Molteno shunt. Notice that several of the devices come in different sizes. The cannula of these devices is placed in the anterior chamber through an ab-externo incision into the angle recess. The large reservoir is placed under the layers of conjunctive and tenon's fascia.
Their postoperative follow-up is highly specialized and frequent adjustments may be necessary postoperatively to maintain proper IOP control.(28),(29),(30)
Combined surgical intervention and pharmacologic enhancement are not uncommon endpoints in eyes that have had multiple procedures.(31)
Figure 15. Cyclodestructive Procedures.

Cyclodestructive procedures (Figure 15) are usually the last resort. The ciliary processes may be partially destroyed by cryopexy, diathermy or by laser either directly or indirectly.(32) Diminution of aqueous production also alters the metabolism and nutritional component of the aqueous humor, which provides nutrients to the lens, iris structures and corneal endothelium.
Treatment of Congenital and Juvenile Glaucoma
Congenital and juvenile glaucoma is often associated with other ocular and even systemic congenital and inherited disorders. In Part I we discussed the presence of aniridia. Cataract, retinopathy of prematurity, microphthalmos, macrophthalmus, strabismus, as well as Reiger-Axenfeld syndrome, are other associated conditions.
Patient Education
As with most diseases, patient education, a lifelong learning process, should be the main focus for patients with glaucoma. Unfortunately, there is little factual knowledge as to how to prevent glaucoma. Nevertheless, in the early stages, if detected by the physician, maintenance therapy can be expected to prevent further damage over a lifetime. In the past ten to fifteen years, largely as a result of newer therapeutic agents with minimal side effects, patient compliance has improved.
The key phrase is "early detection." A visual field that has been lost only very rarely returns. Once damage has occurred, it seems that the optic nerve becomes even more sensitive to IOP fluctuation. Evidence points to further sclerosis and damage to the outflow channels with time and uncontrolled pressure. We suspect there are other factors, as yet unidentified, that affect glaucoma outcomes and are unrelated to intraocular pressure. This is evidenced by further visual field loss in the face of what we used to call normal IOP.
Repetitive reinforcement of the treatment plan at each office visit should include review of medication, proper administration and the following:
- Emphasis on regular examination of the visual field and IOP checks, compliance with medication and proper training of use of eye drops.
- Written material for patient.
- The role of proper diet and exercise in maintaining good health and elimination or reduction of tobacco use.
- The patient should educate and inform their progeny and family about the inheritance of this disorder.
These protocols are especially applicable to geriatric patients who are often forgetful and non compliant. The role of caregivers, family and others is equally important at times.(33)
How to use eyedrops (streaming media will open in a new window.)
Summary
As noted in Part I of this series, early diagnosis of glaucoma, now possible thanks to improved technologies, is an important component of successful glaucoma treatment. Compliance with medical treatment remains, however, a great issue in overall patient management.(34) Treatment selection often is modified by the extent of the disease at the time of diagnosis.(35)
When medical and/or non invasive laser trabeculoplasty fail to control intraocular pressure or progression of the visual field, ophthalmologists will usually recommend trabeculectomy, a non-penetrating procedure. In the United States, trabeculectomy is the procedure of choice.
At present, viscocanalostomy is considered an investigative procedure but this may change with further studies. Tube shunts with any number of devices are reserved for those patients who have failed two or more trabeculectomies with or without adjunctant therapy and for patients with neovascular glaucoma. Neovascular glaucoma is one of the most difficult types of glaucoma to treat successfully and it is often combined with panretinal photocoagulation.