Course Authors
Martin J. Carey, M.D.
Release Date: 11/16/2001
Upon completion of this Cyberounds®, you should be able to:
Discuss the pathophysiology of burn injury
List the classification system for burn injury
Describe the assessment of extent of burn injury
Discuss the management of minor thermal burns in the emergency department.
The focus of this Cyberounds® will be the emergency department management of burns.
Figure 1. Fire and Smoke.

This will include the acute management of major burns, and the acute and on-going management of minor burns.
Each year in the United States, an average of 6,000 people are hospitalized for burns. In addition, more than 60,000 receive attention in emergency departments for burn related injury.
Q. In general, how are burn injuries classified?
A. Burns may be classified into six major groups:
- Scalds
- Liquids
- Splash type injury
- Immersion injury
- Grease
- Steam
- Liquids
- Contact Burns
- Fires
- Flash
- Flame
- Chemical
- Electrical
- Radiation
This discussion will focus on the first three groups.
Q. How are burns graded and what are the characteristics of each grade?
A. Burns are graded as first-, second-, third- or fourth-degree. It is important to note that even experienced examiners often underestimate the depth of a burn on initial presentation.
Figure 2. Cross Section of Skin.
First-degree burns are classically described as red, dry and painful
Figure 3. Sunburn.

Second-degree burns are wet, red and very painful. There is usually blister formation.
Figure 4. Second Degree Burns.

Third-degree burns are dry and leathery in consistency -- the skin is often white and feels hard or waxy. The skin is insensate. These burns will not heal.
Fourth-degree burns involve the deeper tissues, including subcutaneous tissues, tendons and bones.
Figure 5. Deep Third/Fourth Degree Burns.

Q. Who is most at risk from burn injury?
A. It is no surprise that males are more commonly affected than females -- almost two-thirds of all major burn victims are male. Most of these injuries occur during the third decade and reflect the industrial occupational exposure of this group. Minor burns are often encountered in young children and in adults in the third decade. In young children, liquid scalds and hot surface burns (radiators, heaters and 'pot-belly' stoves) are the most common causes.
Serious burns result from flame burns (about one-third) and scalds (about a quarter). About 5% of patients hospitalized with severe burns will die as a result of their injury. The majority of these are from flame burns. It is interesting to note that in building fires at least half of all victims die not from the burns themselves but rather from asphyxiation or from carbon monoxide poisoning.
Q. Emergency physicians often have questions about which children should be managed in a specialized care unit. What are some of the criteria that can be used to help to make this decision?
A. Some of the criteria that indicate that a child should be transferred to a specialized facility include:
- Electrical burns
- Significant chemical burns which compromise function
- Evidence of inhalation injury
- Third-degree burns over more than 5% of the body
- Second- and third-degree burns over 10% or more of the body surface area
- Second- or third-degree burns that involve the hands, face, perineum, genitalia, feet or that cross a major joint.
Other medical or social factors may also influence the decision to transfer. These may include significant intercurrent medical illness, significant trauma associated with the burn, poor home situation, including inability of the caregiver to dress the wounds or a suspicion of abuse or neglect.
Some of these criteria may vary, reflecting local practices. It is a good idea to clarify the exact expectations and requirements of the closest facility. However, these criteria are conservative guidelines.
For adults and children, the American Burn Association grades the level of care required for burns as follows:
Minor burns -- these can be managed on an outpatient basis:
- <10% total body surface area (TBSA) in an adult
- <5% TBSA in young or elderly
- <2% full thickness bur
Moderate burns -- these should be managed on an inpatient basis:
- 10-20% TBSA burn in an adult
- 5-10% TBSA in young or elderly
- 2-5% full thickness burn
- Suspected inhalation injury
- Circumferential burn
- Associated medical problem, e.g., diabetes
Major burns -- these require transfer to a specialized burn center:
- >20% TBSA burns in adult
- >10% TBSA burns in young or elderly
- >5% full thickness burn
- Known inhalation injury
- Significant burn to face, eyes, genitalia or joints
- Significant associated traumatic injury
Q. How may patients be managed as an outpatient after a minor burn?
A. Superficial burns, those without blistering or evidence of deeper skin damage, are best managed simply with a lotion to insure that the skin is moist. Antibiotics are not recommended, as the skin cover is still intact and bacterial invasion is generally not a concern. Burns which have blistered (second-degree burns) should have large blisters, or blisters which have burst, débrided.
Figure 6. Debriding Blisters.

An antibiotic ointment is then applied. Traditionally, this has been silver sulfadiazine. This agent should be avoided on the face (ophthalmic bacitracin is a better choice), if there is a history of sulfa drug allergy, and in the very young, when there is a danger of kernicterus. The ointment is applied twice a day (after the old application is cleaned away) and covered with a gauze dressing.
Newer hydrocolloid dressings are now available. These 'jelly like' dressings are applied, then left in place for about 72 hours. Thereafter, they are changed every 5-7 days. If there is evidence of infection or excessive drainage more frequent application may be required.
Deeper burns that do not require admission should be managed similarly. Close follow-up is required. If infection develops, intravenous antibiotics and inpatient management may be required. Consideration should also be given to the possible benefits of early excision and grafting for some smaller, deep burns, as this can improve healing.
Analgesia is an important aspect of outpatient burn management. Although many patients will get considerable relief from the application of the antibiotic ointment, analgesia is often still required. Analgesia for mild to moderate pain should be used in the first instance, although more extensive burns may require narcotics for a few days initially.
Q. Why use antibiotic ointment in second-degree burns? Why not just wait until infection appears?
A. Burns result in a significant change in the ability of the skin to counter infection. Thus, the use of antibiotics in patients who have a breach in the skin -- those with second degree burns -- is helpful in preventing the development of infection.
Sometimes, patients with even superficial burns will develop infection in the burn. Symptoms usually occur in the first few days after the burn and are characterized by swelling and redness around the burn. The typical organism is Streptococcus pyogenes and it is often highly sensitive to penicillin. Recently, however, Staphylococcus aureus has emerged as a common organism and this organism is often resistant to many antibiotics.
Q. OK, so I can handle the minor burn patient. What about the major burns? How are they best managed in the emergency department? What are the important considerations?
A. The first few hours after a major burn are associated with massive fluid shifts, resulting in profound shock if not corrected adequately. Later, there is a hyperdynamic phase, as the body meets the increased metabolic demands placed upon it. Correct assessment and management during the early phase -- the time when emergency physicians are most likely to be involved in the care of burn patients -- can have a critical impact on patient survival and ultimate recovery of function.
Initially, the patient should be assessed in the usual fashion with attention paid to the airway, breathing and circulation. Burns may have a number of aspects not seen in trauma victims injured by other means. With regard to the airway, burns may cause significant problems with edema and significant burns to the tracheobronchial tree. Maintenance of an adequate airway may require the introduction of an endotracheal tube. This may be required prophylactically with the expectation that edema will occur later. In cases where significant airway compromise already exists, a cricothyrotomy or other invasive airway procedure may be required.
In cases of burns, breathing may be compromised by the presence of circumferential burns around the chest wall. These burns result in restriction of chest expansion and thus respiratory compromise. If this is the case, then an escharotomy should be considered.
Figure 7. Severe Burns with Escharotomies.

Escharotomy is the name given to the procedure of incising through the burnt tissue until healthy tissue is reached. Escharotomies are usually performed with a scalpel or, ideally, with electrocautery. Sedation of the patient is often required, though the tissue itself is usually insensate. Escharotomy of the tissues of the torso is required if there are fully circumferential burns around the chest wall restricting ventilation. Escharotomies may also be limb saving procedures when there are circumferential burns around arms, legs or digits. Swelling under the eschar results in compromise of circulation, unless the pressure is released. In general, escharotomies should be performed on the midlateral or medial aspects of limbs or digits in order to prevent joint exposure. It is important to insure that the eschar is divided through its full length, as even a small remaining area of intact circumferential burn can result in vascular compromise. In addition to escharotomies, fasciotomies are occasionally required if there is significant underlying edema.
Figure 8. Examples of Escharotomies for Limb .

Other aspects important in the immediate management of burn victims include provision of adequate analgesia and sedation as required.
Q. What is the 'rule of nines'?
A. The 'rule of nines' refers to a mechanism to evaluate the extent of the burns. In the adult patient, each 'unit' represents 9% of the total body surface area. Each arm is equal to one unit, each leg, two units, the front of the torso two units and the back two units. The head is one unit. This represents a total of 99% of the body surface area. The remaining 1.0% of the body surface area is allocated to the perineum. Another rule of thumb is that the palm of the hand represents 0.5% of the body surface area. This is useful if there are irregularly shapedburns.
Figure 9. Rule of 9s.
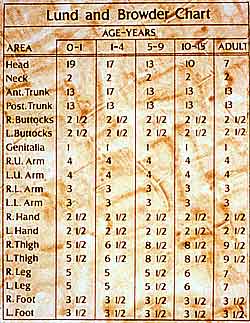
In children, the preferred method of assessment of the extent of the burn area is through the use of the Lund-Browder chart. This chart accounts for the changing body proportions that occur with age. Emergency departments that see pediatric injury should insure that they have a copy of this chart available.
Figure 10. Lund Browder Chart.
Q. What formulae may be used to calculate the fluid requirements of the burn victim?
A. There are a number of different formulae in use in burns centers around the country. Some names are the Evans formula (1 ml/kg/% burn of 0.9% saline + 1 ml/kg/% burn colloid + 2L dextrose 5%) and the Brooke formula (same as above but 1.5 ml/kg/% burn of Lactated Ringer's and 0.5 ml/kg/% burn of colloid). However, the most widely accepted formula is the Parkland formula, which calls for 4 ml/kg/% burn of Lactated Ringer's solution. Half of this volume should be given in the first 8 hours after the burn, while the remaining 50% should be given over the next 16 hours. All of these formulae rely upon monitoring urine output as a guide to adequacy of fluid resuscitation.
Q. Using the Parkland formula discussed above, how would you resuscitate a patient who presents to the emergency department 4 hours after a major burn with second and third degree burns over 70% of the body surface? The patient is a 56-year-old male who weighs 100 kg. He has received a total of four liters of Lactated Ringer's at the referring institution and en route.
A. Using the Parkland formula, the patient requires 4 x 100 x 70 = 28,000 ml of fluid over the first 24 hours. Of this volume, 14,000 ml should be given in the first 8 hours after the burn. So far, the patient has received 4L and, thus, an additional 10 liters need to be given over the next 4 hours at a rate of 2.5 L/hour. Over the next sixteen hours, the patient requires 14L or 875 ml per hour. The patient's urine output will be carefully monitored and additional fluid given if required. The presence of significant inhalation burns will increase the volume of fluids required. Many authorities recommend an increase of 2 ml/kg/% burn if there is significant inhalation injury. Fluid administration should be adjusted to produce 30-50 ml per hour.
In children, it appears that more fluid than calculated according to the Parkland formula might be required. The Shriners' Burn Institute in Texas uses a formula that requires the administration of Lactated Ringer's solution, containing 1.25% salt free human albumin. Over the first 24 hours, 5000 ml/m² burn, plus 2000 ml/m² total body surface area are given. In the same way as the Parkland formula, half of this is given in the first 8 hours and the other half over the remaining 16 hours. Infants may have limited glycogen stores, can become hypoglycemic and may require the addition of glucose infusions. Glucose blood levels should be checked regularly.
Q. When should an inhalation injury be suspected? What are the signs and symptoms?
A. Airway and respiratory complications are a major cause of morbidity and mortality after fires. Careful management of the airway in the emergency department can have a significant impact upon patient survival. Inhalation injury involves the whole of the respiratory tract, from the upper airway down to the alveoli. There may be direct burning of the upper airway from superheated steam or gas. The burns may produce swelling of the airway, which can be further exacerbated by the diffuse capillary leakage secondary to the burn. Irritating gases may produce bronchospasm. The burn directly damages the mucosal layer, destroying the cilia. Later complications of inhalation injury include pneumonia, diminished lung compliance from alveolar collapse and respiratory failure from a combination of all these factors.
The patient with significant inhalation injury may have few signs or symptoms on initial presentation. The emergency physician must maintain a high level of suspicion for inhalation injury. Inhalation injury should be suspected in anyone trapped in a building fire or who lost consciousness during the fire. This is true especially in the presence of heavy smoke. The patient may present with evidence of injury to the upper airway passages, with cough, hoarse voice, stridor or nasopharyngeal irritation. If the injury involves the lower branches of the tracheobronchial tree, then dyspnea, chest discomfort and hemoptysis may be present.
Figure 11. Carbon in ET Tube.

Inhalation injury should be suspected if the patient has evidence of facial or neck burns, singed hair of the eyebrows or in the nose, wheezes, rales, bronchial breathing, cyanosis or if the sputum is soot colored or carbonaceous.
Q. What does the chest X-ray show in inhalation injury? What diagnostic measures should the emergency physician consider when assessing patients with possible inhalational injury?
A. The initial chest x-ray may be normal. After the first 24 hours, however, signs ranging from patchy atelectasis to changes involving the whole lung may be seen.
As noted above, the history and the clinical examination are key diagnostic tools in patients with burn injury. Some authorities believe that emergent bronchoscopy is important to delineate bronchial injury and to clear debris from the larger airways. Consideration should certainly be given to this investigative modality in any patient with a high index of suspicion for inhalation injury.
Small children are particularly at risk for complete airway occlusion. Even relatively minor degrees of mucosal edema can occlude the pediatric airway. Any stridor mandates immediate intubation and this is as true for adults as children. A further reason to do bronchoscopy is that the bronchoscope can function as a stylet, facilitating the introduction of the endotracheal tube under direct vision. This is particularly useful if there is deformed anatomy, significant swelling or intraoral burns.
Occasionally, children will ingest very hot liquids. This produces a very rapid onset of significant edema. The airway may be compromised quickly and these patients should be intubated as soon as possible.
Once the patient is intubated, scrupulous attention should be paid to the maintenance of the airway. All efforts should be made to securely fasten the ET tube in place, to avoid inadvertent removal of the tube, especially in the emergency department where the patient will often be moved around in the course of their immediate assessment. Loss of the airway in these cases can be very serious, as reintubation may be extremely difficult.
If the patient does have bronchospasm because of irritant inhalation, then inhaled bronchodilators are appropriate agents.
A further complication associated with inhalation injury is carbon monoxide poisoning. Carbon monoxide is produced by the combustion of organic material. A carboxy hemoglobin level should be obtained on all patients with a history of burns. In general, if the level of carboxy hemoglobin is between 0 and 10%, there will be minimal symptoms. In fact, many smokers, especially heavy smokers, will have levels approaching 10%. Between 10 and 20% of patients may experience nausea and a significant headache, often described as pounding. Drowsiness occurs at levels between 20 and 30% and the patient may experience weakness. Above 30%, confusion and agitation are common. If over 40%, the patient will often be comatose with respiratory depression. Death occurs at levels above 50%. It must be noted, though, that these levels are only guidelines and patients may have experienced significant carbon monoxide exposure, but have lower levels by the time they reach tertiary care.
Carbon monoxide affects oxygen transport mechanisms and the utilization of oxygen by the mitochondrial cytochrome oxidase system. Carbon monoxide can be cleared from the hemoglobin molecule before the cytochrome oxidase system. The management of acute carbon monoxide poisoning is the administration of 100% oxygen. In room air, the half-life of carboxyhemoglobin is about 240 minutes. In the presence of 100% oxygen, this falls to 30 to 40 minutes. If the patient has significant carboxyhemoglobin levels -- above 20-30% -- they should receive 100% oxygen and this is best administered via an endotracheal tube. Treatment should continue until the patient no longer exhibits a metabolic acidosis. Some authorities recommend the use of hyperbaric oxygen for the treatment of carbon monoxide poisoning but firm evidence of its utility is lacking. In addition, the provision of intensive care to an unstable patient in most hyperbaric facilities is difficult.
Other agents present in smoke may cause significant irritation and bronchospasm. These include benzenes, aldehydes, ammonia, acrolein and nitrogen oxide. Hydrogen cyanide may also be produced from the combustion of wool and plastics. Exposure to hydrogen cyanide gas should be considered in patients presenting with respiratory failure with no other obvious cause.
Q. What can the Emergency Physician do to help prevent burns?
A. There are a number of risk factors associated with burn injuries. In particular, low socioeconomic status has been identified as a major risk. In a study from New York State, for every $1000 drop in income there was an increase of 49 burns per 10,000 person years. Black children have three times the risk of suffering a serious burn than do white children. Children in single parent homes are also at increased risk.
House fires are the main cause of burns to children and cigarettes are a major factor in these fires. Physicians can help prevent some of these burns by educating parents about the dangers, especially insuring that elderly smokers who live in the household are aware of the dangers.
Physicians can also be advocates for smoke detector programs. The presence of a functioning detector has been shown to decrease the risk of death in a fire by 60%. Discussing the importance of smoke detectors with parents as part of a child health surveillance consultation has been shown to increase use of smoke detectors. Community based smoke detector 'give away' programs also reduce the incidence of fire related injuries. It is estimated that the presence of a smoke detector results in an 80% reduction in mortality and a 74% reduction in injuries from domestic fires. Physicians can become involved in these community-based programs, and thus increase awareness and reduce burn-related injuries in the community.
Physicians can also help by educating parents and children about the importance of an escape plan, which is practiced regularly by all family members. This advocacy can occur through church or community based groups, or through the schools. The use of the 'stop, drop, roll' program to teach children what to do if they should ever find their clothing ablaze has also had a positive impact on survival.
Another major cause of burns in the home is scalds from hot water taps. If water is at 158°F (70°C), full thickness burns occur in about one second. At 131°F (55°C), it takes about 30 seconds for a full thickness burn. At 120°F (49°C), it takes ten minutes. Thus, experts advise that the water heater should be set at less than 120°F. A meat thermometer, present in many homes, can be used to gauge the water temperature if it is held under the running hot water tap. Physicians should be aware of these figures and advise their patients accordingly.
Q. What particular types of burns should emergency physicians be particularly aware of in children (or in elderly people)?
A. Burns can sometimes be indicative of abuse. Warning signs may include an injury that is reported as self-inflicted or caused by another sibling; a situation where the mechanism described seems beyond the capacity that would be expected of a child of that age; or an instance where the mechanism of injury described does not seem to fit with the pattern of injury noted. It is important to note that a number of these factors are common to all types of non accidental injury, as are delayed presentation, a history of previous abuse or the arrival of the child with a person who is not the regular caregiver.
Circular burns, often described as 'punched out,' are indicative of burns from cigarettes. Scald injuries can be seen as a sign of abuse. Typically, these burns spare the flexor creases, as the child is 'curled up' in a protective posture. Burns that have a well demarcated line around the buttocks, feet (especially just the heels) and the perineum are indicative of a child being lowered into scalding water and are highly suspicious of abuse. Emergency physicians should be aware of these patterns of injury. Unfortunately, elder abuse is being recognized more and more. They too may show circular cigarette burns.