Course Authors
Meera B. Chitlur, M.D.
Dr. Chitlur is Associate Professor, Wayne State University School of Medicine, and Director, Hemophilia Treatment Center and Hemostasis Program, Division of Pediatric Hematology/Oncology, Children's Hospital of Michigan, Detroit, MI.
Within the past 12 months, Dr. Chitlur has been a consultant to Bayer HealthCare and Novo Nordisk.
Albert Einstein College of Medicine, CCME staff, and interMDnet staff have nothing to disclose.
This activity is certified for hematologists, HEM/ONCs, surgeons, anaesthesiologists, intensivists, hospitalists, critical care medicine specialists, emergency medicine clinicians, PCPs and other healthcare providers interested in managing hospitalized patients with bleeding disorders.
This CME activity has been peer-reviewed by Henny H. Billet, M.D., Professor of Clinical Medicine, Department of Medicine (Hematology), Professor of Clinical Pathology, Department of Pathology, Chief, Division of Hematology, Department of Medicine, Albert Einstein College of Medicine, Montefiore Medical Center, Bronx, NY.This activity is made possible by an unrestricted educational grant from Novo Nordisk

Estimated course time: 1 hour(s).

Albert Einstein College of Medicine – Montefiore Medical Center designates this enduring material activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through joint sponsorship of Albert Einstein College of Medicine of Yeshiva University and Educational Concepts in Medicine. Albert Einstein College of Medicine of Yeshiva University is accredited by the ACCME to provide continuing medical education for physicians.
Upon completion of this Cyberounds®, you should be able to:
Review the clinical presentation and laboratory diagnoses to appropriately diagnose unexplained or unusual bleeding in hospitalized patients
Employ evidence-based treatment modalities for hemostatic control of bleeding and inhibitor eradication in patients with AHA or other unexplained bleeding
Discuss treatment advances for RBDs including new and emerging recombinant products.
This presentation may include discussion of commercial products and services.
|
Case History and Lab Results A 65-year-old man is hospitalized for cerebellar infarction. At admission, he was drowsy, without clinical evidence of bleeding. He was administered aspirin, clopidogrel and valproate for cerebellar infarction; a statin for hyperlipidemia; and clindamycin and teicoplanin for aspiration pneumonia. Following intubation, a tracheostomy was performed. Bleeding history: No previous familial medical history of bleeding or coagulopathy; no clinical symptoms or signs of malignancy, antiphospholipid syndrome or collagen vascular disease. Initial laboratory results: Normal CBC, kidney and liver function, and coagulation parameters. Three weeks after initiation of clopidogrel, blood begins oozing from tracheostomy site and aPTT is prolonged at 40.3 s (reference range 27.9-37.8 s). PT and PLT count are within normal range. Course of action: Clopidogrel discontinued, as this is believed to be the cause of bleeding. Nevertheless, blood continues to ooze from the tracheostomy stoma, and the aPTT gradually rises to 98.8 s without platelet or PT changes, despite discontinuation of clopidogrel and a transfusion of FFP. Source: Adapted from Hwang et al.(1) |
Given the approximately 36.5 million hospital admissions in the United States,(2) this scenario could very well be one that you are required to manage someday. Would you know how to handle it?
Overview
Numerous bleeding etiologies are encountered in the intensive care unit, including inherited and acquired disorders such as von Willebrand disease (vWD), platelet disorders, thrombocytopenia and disseminated intravascular coagulation (DIC).(3) While some disorders are more readily apparent than others, not all bleeding is straightforward or has a readily identifiable cause. Unexplained bleeding includes patients who present with either unrelenting bleeding, unusual sites of bleeding or life-threatening hemorrhage.(4) Moreover, bleeding that is unprovoked, is of unexpected volume, or occurs from unexpected or multiple sites suggests the possibility of new onset or a previously unrecognized systemic bleeding disorder.(4)
The management of patients with unexpected bleeding should be based on clinical scenario, thorough physical exam, and results of screening or specific laboratory tests.(4) To recognize new-onset or acquired syndromes, in particular, the clinician must maintain a high index of suspicion.(4)
The challenge of unexplained bleeding lies in its identification—putting a name to the hematologic disturbance. The hematologic disturbances featured in this Cyberounds® include acquired hemophilia (AH) because of its high rates of morbidity and mortality, acquired factor XIII (FXIII) deficiency because it is associated with significant mortality,(5) and congenital FVII deficiency because it is the most common of the rare bleeding disorders (RBDs).(6) These three bleeding disorders are not readily apparent but could be encountered by both hematologists and non-hematologists who may very well ask, "Is it AH or something else"?
Acquired Hemophilia A
Background and Epidemiology
AH is a rare condition caused by the production of autoantibodies against FVIII. Both men and women are equally affected, as there is no known genetic inheritance pattern.(3) (7) AH has a worldwide prevalence and appears in all ethnic groups.(8) The condition typically presents in middle and older age and rarely arises in childhood.(8) (9) Up to 90% of affected patients experience a severe bleeding diathesis.(3)
AH has an annual incidence of 1.5 cases/million,(10) making it rarer than congenital hemophilia, which has an estimated frequency of 1/10,000 births.(11) The disorder has a biphasic age distribution, with an increased incidence among those aged 65 and older and a small increase in incidence among postpartum women due to its association with pregnancy.(3) (12) (13) The disorder is often not recognized or is mistaken for other acquired bleeding disorders.(8) (14)
Diagnosing AH can be difficult because of its association with other conditions. Although 50% of cases are labeled idiopathic,(7) it is associated with various other disease states or conditions in another 50% of cases. Frequent associations include autoimmune diseases, solid tumors and lymphoproliferative diseases, as well as certain medications (see Table 1).(9) (11) (15)

Table 1. Conditions Associated With Acquired Hemophilia.
| Condition | Comments |
|---|---|
| Pregnancy | AH usually occurs 1-4 mo after delivery; possible recurrence in subsequent pregnancies. |
| Autoimmune disease | An autoimmune disease association has been suggested in 17%-18% of AH patients, including rheumatoid arthritis, systemic lupus erythematosus, Sjögren's syndrome, dermatomyositis; rarely, myasthenia gravis, multiple sclerosis, Grave's disease, autoimmune hemolytic anemia |
| Malignant neoplasm | Up to 10% of AH patients have underlying malignancy (especially hematologic) |
| Drug-related | Several medications are associated with AH, including antibiotics (penicillin, sulfonamides, chloramphenicol), anticonvulsants (phenytoin), methyldopa, interferon-α, clopidogrel, fludarabine |
Source: L. Brunetti et al.(12) By permission of the authors.
Clinical Manifestations
The most common presenting symptom of AH is unexplained excessive bruising and bleeding in patients older than 60.(12) When the skin is involved, ecchymoses may be diffuse, involving the entire limb or large areas of the chest or abdomen. The classical presentation is purpura or soft tissue bleeding (see Figure 1).(7) (10)
Figure 1. Typical Presentation of AH.
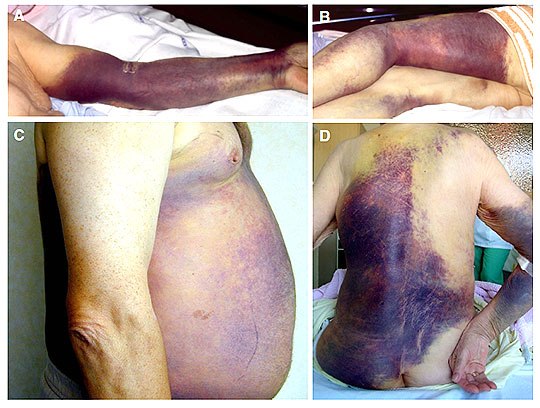
Source: P. Collins et al.(10) By permission of the authors.
Other manifestations of AH include severe muscle bleeding, hematuria, urogenital tract bleeding, compartment syndrome, GI bleeding, epistaxis and intracerebral bleeding.(7) (10) (13) Bleeding is often spontaneous, and severity does not correlate with FVIII level or strength of inhibitor.(10) Fatal hemorrhages occur in 9% to 22% of cases, and mild bleeding in approximately 30% of cases.(10) (16)
Laboratory Evaluation and Differential Diagnosis
Diagnosis requires clinical acumen and sophisticated laboratory evaluation.(7) Early diagnosis is characterized by an isolated prolonged activated partial thromboplastin time (aPTT), the most common screening abnormality, with a normal prothrombin time (PT), thrombin time (TT) and platelet count, as well as low FVIII levels.(7) (12) (13) These findings will automatically rule out other common causes of bleeding in hospitalized patients (see Table 2).(3)
Table 2. Typical Diagnostic Laboratory Findings for Coagulation Disorders.
| Condition | Platelet count | aPTT | PT | Fibrinogen | Fibrin degradation products | D-dimer | Thrombin time |
|---|---|---|---|---|---|---|---|
| DIC | Decreased | Prolonged | Prolonged | Decreased | Positive | Positive | Prolonged |
| Liver failure | Low/ normal |
Prolonged | Prolonged | Low/ normal |
Negative | Negative | Prolonged |
| Vitamin K deficiency | Normal | Normal /prolonged |
Prolonged | Normal | Negative | Negative | Normal |
| Acquired hemophilia | Normal | Prolonged | Normal | Normal | Negative | Negative | Normal |
| Heparin effect | Normal | Prolonged | Normal | Normal | Negative | Negative | Prolonged |
| Abnormal platelet function | Normal | Normal | Normal | Normal | Negative | Negative | Normal |
Source: A. Shander et al.(3) By permission of the authors.
It is important to differentiate AH from other disorders. It can easily be confused with DIC, which would normally present with thrombocytopenia and a prolonged PT and aPTT.(7) vWD, too, should be ruled out. This disorder is the most common hereditary coagulation abnormality, with a 0.01% prevalence in the general population.(17) Finally, it is important to rule out nonspecific inhibitors [i.e., heparin or lupus anticoagulant (also known as lupus antibody or LA)] that could prolong the aPTT.(7) It is especially critical to distinguish between FVIII inhibitors and antiphospholipid antibodies, such as LA, because they may artificially lower FVIII, thereby mimicking AH.(12) Figure 2 depicts an algorithm for the differential diagnosis of an isolated prolonged aPTT:(10)
Figure 2. Algorithm to Guide the Management of Patients With Suspected Acquired Hemophilia.
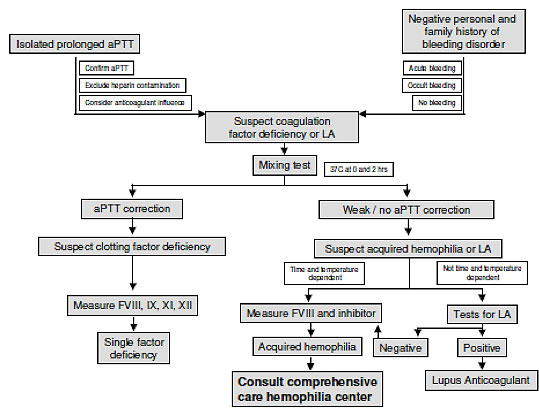
Source: P. Collins et al.(10) By permission of the authors.
A mixing study is the most common way to further delineate the cause of an isolated prolonged aPTT and distinguish AH from other disease states.(7) (12) (13) The technique involves the mixing of normal plasma with equal volumes of patient plasma. The aPTT of the mixture should correct to within 4 seconds of the normal plasma aPTT if there is a clotting factor deficiency; in the presence of an inhibitor, it will not correct. Because an inhibitor is time- and temperature-dependent, the mixture should be incubated for at least 1 hour at 37°C.(13) (15) The aPTT should be measured in the normal control and patient/normal mixed sample both immediately and after incubation for 2 hours (a difference of 5 seconds or greater is indicative of an inhibitor). See Table 3.
Table 3. aPTT at 37°C With Various Incubation Mixtures.(13)
| Incubation mixture | 15 minutes | 30 minutes | 1 hour | 2 hours |
|---|---|---|---|---|
|
Normal plasma plus
Factor VIII-deficient plasma |
37 | 37 | 41 | 45 |
| Weak inhibitor (1 BU) | 37 | 38 | 45 | 53 |
| Moderate inhibitor (5 BU) | 43 | 47 | 55 | 64 |
| Strong inhibitor (20 BU) | 54 | 61 | 77 | 92 |
| Normal plasma alone | 32 | 32 | 36 | 40 |
Treatment
The management of AH is two-pronged: arrest bleeding and eradicate inhibitor while treating the underlying cause. Most patients require immediate treatment to control bleeding,(10) although there is no established treatment protocol because there are insufficient new cases to generate high-level evidence for any treatment regimen.(15)
International guidelines recommend two interventions for hemostatic control: bypassing agents (aPCC; rFVIIa) or FVIII concentrates and desmopressin to increase FVIII levels.(15) Inhibitor titer is used as a guide to determine treatment strategy, although it must be kept in mind that titer does not always reflect the potency of an inhibitor (some clinicians, such as Shander,(3) believe the severity of the hemorrhage should guide treatment decisions).
For low-titer inhibitors (<5 BU/mL), the primary strategy comprises high doses of FVIII concentrate with or without desmopressin to increase circulating levels of FVIII.(3) For high-titer inhibitors (??JPY5 BU/mL), bypassing agents are considered the primary treatment of choice, based on the results of numerous studies, as well as clinical experience, which demonstrate the efficacy of these agents in approximately 90% of patients.(18) (19) (20) (21) Table 4 outlines treatments and dosing regimens.
Table 4. Dosing of Treatments for AH With Active Bleeding.
| Dosing treatments | Dose regimen |
|---|---|
|
Restoration of hemostasis
Treatments that increase circulating levels of factor VIII
|
|
|
Human factor VIII concentrates |
40 IU/kg IV plus 20 IU/kg IV for each BU of inhibitor |
|
Desmopressin |
0.3μg/kg IV/SC |
|
Bypassing agents |
|
|
rFVIIa |
70-90 μg/kg IV every 2-3 h until response is observed |
| pd-aPCC | 50-100 U/kg every 6-12 h until response is observed (maximum of 200 U/kg/day) |
| Mucous membrane bleed: 50 U/kg every 6 h; increase to 100 U/kg every 6 h for persistent bleeding Serious soft tissue or other severe bleed: 100 U/kg every 12 h |
Source: A. Shander et al.(3) By permission of the authors.
Once bleeding is arrested, immunosuppressant treatment is required to curb and eventually eliminate inhibitor formation.(8) Although spontaneous remission has been noted to occur in up to one-third of patients, this occurrence is variable, and it cannot be known for certain which patients will achieve remission.(3) Therefore, long-term inhibitor suppression is required.
While the optimal strategy remains undefined,(15) prednisolone is considered the usual therapeutic agent; azathioprine is an alternative immunosuppressant. Mycophenolate and cyclosporine are also prescribed, while rituximab has proven effective in patients resistant to first-line therapy or for whom steroids and/or cytotoxics are contraindicated.(15) Because relapse is observed in as many as 20% of patients, extended follow-up of approximately 24 months is required.(8)(10) Table 5 provides a breakdown of strategies for inhibitor eradication.(15)
Table 5. Inhibitor Eradication Treatment Strategies in AH.
| First-line treatment |
|---|
| Corticosteroids Corticosteroids + cyclophosphamide |
| Second-line treatment |
| Rituximab |
| Alternative treatment |
| Azathioprine Vincristine Mycophenolate Cyclosporine |
| Not recommended |
| Intravenous immunoglobulins |
Source: A. Huth-KA 1/4 hne et al.(15) By permission of the authors.
Acquired FXIII Deficiency
Background and Epidemiology
Acquired FXIII deficiency is an extremely rare bleeding disorder, with only 28 reported cases.(5) However, it is associated with significant mortality—29%. The rate increases to 60% in patients presenting with cerebral hemorrhage. Both men and women may be affected, although there is a slight predominance in women, with a male/female ratio of 0.9.(22) Most patients present at an older age, and its occurrence in pediatric patients is rare. Cases are typically associated with an acquired IgG inhibitor against FXIII.
FXIII is important to clot formation and is the last enzyme to be activated in the blood coagulation pathway, at which point it is converted by thrombin and Ca2+ into an active transglutaminase (FXIIIa).(23) Besides mechanically stabilizing fibrin clots, activated FXIII is essential to wound healing, angiogenesis and the maintenance of pregnancy.(22) Researchers suspect that it plays a role in the maintenance of vascular permeability, stabilization of bone and cartilage extracellular matrix and cardioprotection. Although the disorder can be idiopathic, especially in elderly patients, it is reported to be associated with several conditions or diseases (Table 6).(24)
Table 6. Conditions Associated With Acquired FXIII Deficiency.(5)(22)
| Condition | Comments |
|---|---|
| Autoimmune Disorders | Systemic lupus erythematosus, rheumatoid arthritis, diabetes mellitus |
| Other Disorders | IBS, leukemia, malignancies, stroke, PE, cirrhosis, sepsis, immune thrombocytopenic purpura |
| Drug-Related | Isoniazid, phenytoin, penicillin, procainamide, practolol, ciprofloxacin, amiodarone |
Clinical Manifestations
In acquired FXIII deficiency, the bleeding diathesis is often severe.(22) Frequent symptoms include spontaneous severe subcutaneous and retroperitoneal bleeding, spontaneous or posttraumatic hematomas, postoperative bleeding and cerebral hemorrhage.(24) Frequently, the initial presenting symptom is postsurgical or postdental extraction hemorrhages.
Laboratory Evaluation
Inhibitors should be suspected by the sudden appearance of severe hemorrhagic symptoms in patients with normal routine coagulation assays and a personal/family history negative for bleeding complications.(25) (26) (27) Further evaluation is required if FXIII deficiency is suspected. The clot solubility test is the most widely used and readily available.(28) Historically, the laboratory hallmark of acquired FXIII deficiency was the increased solubility of a patient's clot in 5 M urea or 100% monochloroacetic acid. However, this test has several limitations: It only detects severe deficiencies; it is not standardized; its sensitivity depends on fibrinogen level, clotting reagent, and the particular solubilizing agent and its concentration; its detection limit varies between <0.5% and 5% FXIII activity.(29) For these reasons, it is no longer recommended.(25)
For an accurate diagnosis, quantitative assays are required and should be used as a first-line method of detection.(29) Their use is based on two assay principles: measurement of ammonia released during transglutaminase reaction and measurement of labeled amine incorporated into a protein substrate.(26) The three types of quantitative assays include amine incorporation, ammonia release and FXIII antigen assays.
Inhibitors are confirmed by a mixing study according to Bethesda assay or Nijmegen modification. The Bethesda assay is used for identifying and quantifying clotting factor inhibitors. It involves the incubation of patient plasma with normal plasma for 2 hours at 37°C, and the residual clotting factor is then measured. A 50% decrease in the original concentrate defines one Bethesda unit of inhibitor.(30) This method has undergone a modification (Nijmegen) to include buffers to minimize shifts in pH, thereby improving accuracy.(30) Either of these studies determines whether the deficiency is congenital or acquired.(22) With a congenital deficiency, mixing usually corrects plasma; in the presence of an inhibitor, there is no correction.
Treatment
Similar to AH, the management of acquired FXIII deficiency comprises treatment of the acute hemorrhage and its complications by increasing activity of the deficient factor and eliminating the inhibitor.(31) Historically, patients were treated with whole blood, FFP and cryoprecipitate; however, these rarely improved activity of FXIII.(22)
While there is no consensus on current management strategies for this disorder, it is typically treated with plasma-derived FXIII concentrates.(5) In the United States, Corifact® is the only licensed concentrate available. Based on a systematic review of patients with acquired FXIII deficiency, Franchini and colleagues determined that doses of 50-150 U/kg produced adequate hemostasis. An investigational treatment of recombinant FXIII (rFXIII-A2) currently awaits FDA approval.(32) Other treatments include rFVIIa and antifibrinolytic agents, but further studies are needed to determine their efficacy for this disorder.(31) (33)
Inhibitor eradication strategies include plasmapheresis or immunoadsorption with staphylococcal protein A, immunosuppression with cyclophosphamide and/or corticosteroids, infusion of immunoglobulins and rituximab.(22) (31)
Congenital FVII Deficiency
Background and Epidemiology
FVII deficiency is the most common of the RBDs, with an estimated prevalence of 1:300,000 to 1:500,000 population.(34) (35) Prevalence is higher in countries where consanguineous marriage is frequent. In most patients, the disorder is mildly hemorrhagic, characterized by mucous membrane and skin bleeds, including epistaxis, menorrhagia, gum bleeding and easy bruising.(36) Patients with severe deficiency become symptomatic at a young age (i.e., soon after birth or as toddlers).
A distinguishing and intriguing feature of FVII deficiency is its clinical heterogeneity.(37) Symptoms can range from mild to severe, with no clear or consistent correlation between circulating FVII and clinical manifestations. It is not uncommon for an individual with low levels of FVII activity (<1%) to manifest no bleeding symptoms, while an individual with levels greater than 5% may have a personal history of severe bleeding symptoms.
Several FVII registries have helped to shed light on this rare and clinically unpredictable disease: the International Registry on Congenital FVII Deficiency (IRF7), now closed, is currently analyzing more than 500 patient entries. Most recently, the Seven Treatment Evaluation Registry (STER), just closed in 2012, is analyzing data from its postmarketing data collection system, reviewing efficacy and safety data, incidence of thrombosis, inhibitor formation and treatment strategies.
The combined data from these registries yield more than 750 evaluable cases of FVII deficiency. Based on their findings, a composite picture of the bleeding diathesis for this disorder emerges. Three bleeding phenotypes have been observed: asymptomatic, platelet-like (mucocutaneous bleeding) and hemophilia-like (life- or limb-threatening severe bleeding). The relationship between residual clotting activity and disease severity is not clear, although according to registry findings, the first major bleeding symptom is an independent predictor of the risk of subsequent major bleeds.(38)
Clinical Manifestations
The most common symptoms of FVII deficiency are mild and include hemorrhage of mucous membrane and skin, as well as epistaxis.(39) CNS or GI bleeding occurs in 20% of patients, and life-threatening bleeds occur most frequently (65%-70% of cases) during the first six months of life (see Figure 3).(40) In newborns, CNS, GI, cephalohematoma and umbilical bleeding are most common.
Figure 3. Ranking of Symptoms by Age at Presentation.
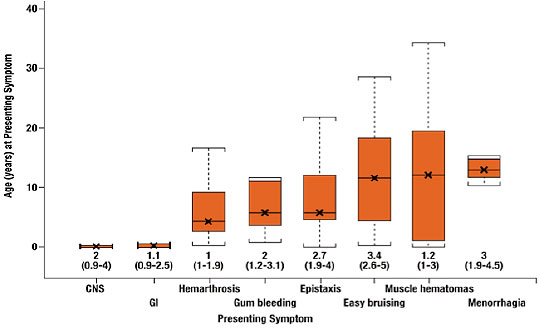
Source: G. Mariani et al.(*) By permission of the authors.
Laboratory Evaluation
FVII deficiency can be suspected when hemostatic screening reveals an isolated prolongation of the PT with a normal aPTT. While the FVIIc assay is readily available and an important test to further confirm diagnosis, there are difficulties associated with its use because the test is highly dependent on thromboplastin sensitivity. Recently, global assays of coagulation and fibrinolysis have been found to correlate with FVII:c.(41) These tests, including clot formation and lysis (CloFAL), simultaneous thrombin and plasmin generation (STP) assays, thrombin generation assays and thromboelastography, may provide a better assessment of bleeding tendency but further evaluation is needed.(42)
Treatment
Low-dose rFVIIa (15-30 µg/kg bw) is considered the optimal replacement therapy for FVII deficiency. FFP is also an option, but with limited use, primarily in developing countries where no other treatments are readily available, as it carries the risk of volume overload and transmission of blood-borne viruses. Plasma-derived FVII concentrates represent another option. Unlike FFP, they carry a lowered risk for transmission of blood-borne pathogens because of viral inactivation methods. Prothrombin complex concentrates have also been used to treat FVII deficiency but carry a risk for posttreatment thrombosis.(43)
Prophylaxis
Although little is known about the use of prophylaxis to treat FVII deficiency, it is viewed as a promising treatment option, despite the short half-life of infused FVII. Newborns who experience early and severe CNS or GI bleeding are the main target, as are toddlers, based on results of STER, which suggest that primary prophylaxis be mandatory in children younger than two years and in toddlers with a high bleeding risk. The suggested prophylactic regimen is rFVIIa three times per week, 90 µg/kg bw total weekly dose.(34)
|
Subsequent testing: Mixing test performed and aPTT remained uncorrected. Tests for lupus anticoagulant, anticardiolipin antibody, and antinuclear antibody were negative. The patient's FVIII level was <1% (reference range 60%-140%), and the FVIII inhibitor titer was 5.4 BU/mL. Diagnosis and next steps: Patient was believed to have medication-associated AH as a result of the clopidogrel he had been administered. Steroids were given, and within several days, bleeding control was achieved and the patient's aPTT returned to normal levels. However, several weeks following steroid use, active bleeding from the stoma developed. The aPTT was normal, the FVIII inhibitor was undetectable, and the FVIII level was 8%. A left inferior thyroid arterial branch ligation was performed and bypassing therapy with rFVIIa administered. No further bleeding episodes developed. FVIII levels eventually normalized after 2 months of treatment. The patient was tapered off steroids, and bypassing therapy was discontinued. During two years of follow-up, his aPTT remained within normal limits. Case Conclusions The diagnosis of AH requires a high index of clinical suspicion. Appropriate laboratory evaluation and rapid initiation of treatment with hemostatic agents and immunosuppressive therapy are essential. Although in the case described above, the initial treatment only included steroids, it is recommended that bypassing therapy be initiated immediately to control bleeding, along with immunosuppressive therapy.(9) Given the lack of laboratory assays to assess treatment efficacy, AH remains a management challenge. Global hemostatic assays such as thrombin generation and thromboelastography may, potentially, be useful, as they enable the clinician to evaluate the hemostatic profile. Significant deficits still exist in our understanding of the pathophysiology of this disease. Successful inhibitor eradication is key to managing the bleeding and preventing life-threatening and fatal bleeds. Since AH is more commonly seen in the elderly, the risk of complications such as sepsis, neutropenia, diabetes and psychiatric illnesses secondary to immunosuppression is extremely high. As a rare disease, with only observational data currently available, randomized controlled trials are not likely. |
Summary
Clinicians should consider the possibility of an acquired bleeding disorder or previously unrecognized congenital bleeding disorder when presented with unprovoked or unexplained bleeding in patients. Putting a name to these hematologic disturbances requires clinical acumen and the ability to interpret laboratory tests.
Further laboratory investigations are warranted in cases in which routine coagulation tests are normal in the presence of persistent and/or unprovoked bleeding. As additional information comes to light about the less frequently encountered acquired or congenital factor deficiencies, particularly AH, acquired FXIII deficiency and congenital FVII deficiency, it is hoped that evidence-based treatment guidelines can begin to be formulated to improve patient outcomes.